Download

1 / 14
140 likes | 271 Views
Classifying seronegative MG: A population based study. A Carr 1,4 , MI Leite 2 , A Vincent 2 , C Cardwell 3 , P McCarron 3 , D O’Reilly 3 , J McConville 1,4 Department of Neurology, Royal Victoria Hospital, Belfast, Northern Ireland.

E N D
Classifying seronegative MG:A population based study A Carr1,4, MI Leite2, A Vincent2, C Cardwell3, P McCarron3, D O’Reilly3, J McConville1,4 Department of Neurology, Royal Victoria Hospital, Belfast, Northern Ireland. Neurosciences Group, John Radcliffe Hospital, University of Oxford, UK 3. Department of Medical Statistics and Epidemiology, Queens University, Belfast, Northern Ireland. 4. Department of Neurology, Ulster Hospital Dundonald, Belfast, Northern Ireland
Aims • Describe the epidemiology of MG in Northern Ireland • Classify cases by serological subtype • Assess the usefulness of recently developed techniques
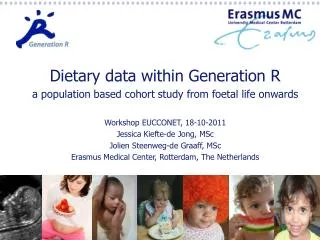
Methods • Multiple sources of case ascertainment • Study period: 01/01/2000 – 31/12/2008 • Clinical confirmation and serological classification of individual cases • Characterisation by age, sex, symptomatology, diagnosis, treatment and co-morbidities
Results • 717 possible cases • 287 excluded • 342 prevalent cases (31/12/2008) • Ascertainment= 98.2% (95%C.I.: 92.1, 99.6) • 212 incident during study period • 186 AChR MG • 26 SNMG
Serological analysis • 23 SNMG • 12 AChR MG • 6 MuSK MG • 4 Healthy controls (HC)
AChR+rapsyn-EGFP EGFP Serum+ anti-human IgG Serum+ anti-human IgG
Cell-based immunofluorescent assay: MuSK Serum+ anti-human IgG MuSK-EGFP Merged Case Case Control
Cell-based immunofluorescent assay: clustered AChR AChR+rapsyn-EGFP Serum+ anti-human IgG Merged Case Case Control
Characteristics of serological subgroups No difference. ANOVA; p: 0.065 No difference. 2; p>0.5 No difference. ANOVA; p: 0.898 No difference. ANOVA; p: 0.393
Conclusions • Cell based assays improve serological classification of autoimmune MG • A proportion of cases remain seronegative
Acknowledgements Prof Angela Vincent, Neurosciences group, Oxford University Dr Isabel Leite, Neurosciences group, Oxford University
Neuromuscular junction • AChR ab in 80% • MuSK ab in 10% • SNMG 10% Motor neurone Muscle end plate Acetylcholine receptor MuSK Dok-7 Rapsyn Acetylcholine vesicle Pre-synaptic Ca2+ channel