Download
1 / 1
10 likes | 143 Views
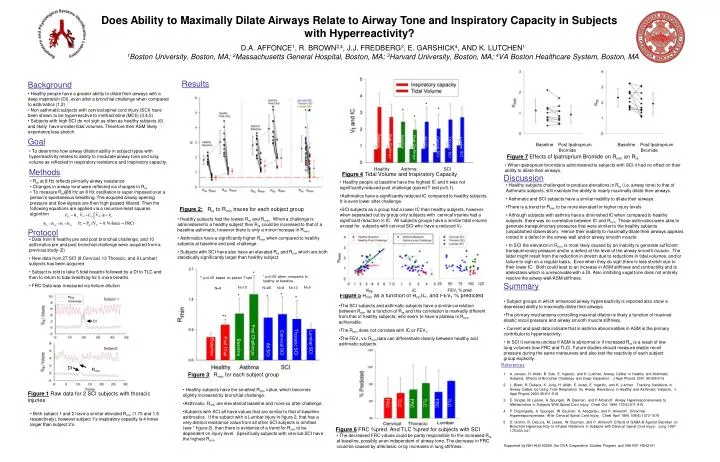
Does Ability to Maximally Dilate Airways Relate to Airway Tone and Inspiratory Capacity in Subjects with Hyperreactivity?. D.A. AFFONCE 1 , R. BROWN 2,4 , J.J. FREDBERG 3 , E. GARSHICK 4 , AND K. LUTCHEN 1

E N D
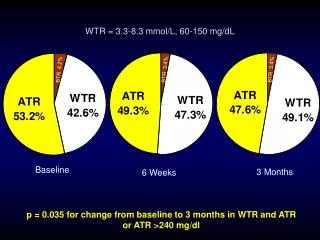
Does Ability to Maximally Dilate Airways Relate to Airway Tone and Inspiratory Capacity in Subjects with Hyperreactivity? D.A. AFFONCE1, R. BROWN2,4, J.J. FREDBERG3, E. GARSHICK4, AND K. LUTCHEN1 1Boston University, Boston, MA; 2Massachusetts General Hospital, Boston, MA;3Harvard University, Boston, MA; 4VA Boston Healthcare System, Boston, MA Results Background • Healthy people have a greater ability to dilate their airways with a deep inspiration (DI), even after a bronchial challenge when compared to asthmatics (1,2) • Non asthmatic subjects with cervical spinal cord injury (SCI) have been shown to be hyperreactive to methacholine (MCh) (3,4,5) • Subjects with high SCI do not sigh as often as healthy subjects (6) and likely have smaller tidal volumes. Therefore their ASM likely experience less stretch. * * * * * Baseline Post Challenge Baseline Post Challenge Goal All SCI Cervical SCI Thoracic SCI Lumbar SCI Baseline Post Ipatroprium Bromide Baseline Post Ipatroprium Bromide * • To determine how airway dilation ability in subject types with hyperreactivity relates to ability to modulate airway tone and lung volume as reflected in respiratory resistance and inspiratory capacity. Figure 7 Effects of Ipatroprium Bromide on Rmin an Rrs • When ipatroprium bromide is administered to subjects with SCI it had no effect on their ability to dilate their airways. Healthy Asthma SCI Methods Figure 4 Tidal Volume and Inspiratory Capacity Discussion • Rrs at 8 Hz reflects primarily airway resistance • Changes in airway tone were reflected via changes in Rrs • To measure Rrs@8 Hz an 8 Hz oscillation is super imposed over a person’s spontaneous breathing. The acquired airway opening pressure and flow signals are then high passed filtered. Then the following equations are applied via a recursive least squares algorithm • Healthy people at baseline have the highest IC and it was not significantly reduced post challenge (paired T test p>0.1). • Asthmatics have a significantly reduced IC compared to healthy subjects. It is even lower after challenge. • SCI subjects as a group had a lower IC than healthy subjects, however when separated out by group only subjects with cervical injuries had a significant reduction in IC. All subjects groups have a similar tidal volume except for subjects with cervical SCI who have a reduced VT • Healthy subjects challenged to produce elevations in Rrs (i.e. airway tone) to that of Asthmatic subjects, still maintain the ability to nearly maximally dilate their airways. • Asthmatic and SCI subjects have a similar inability to dilate their airways. • There is a trend for Rmin to be more elevated for higher injury levels • Although subjects with asthma have a diminished IC when compared to healthy subjects there was no correlation between IC and Rmin. These asthmatics were able to generate transpulmonary pressures that were similar to the healthy subjects (unpublished observation). Hence their inability to maximally dilate their airways appears rooted in a defect in the airway wall and/or airway smooth muscle • In SCI the elevation in Rmin is most likely caused by an inability to generate sufficient transpulmonary pressure and/or a defect at the level of the airway smooth muscle. The latter might result from the reduction in stretch due to reductions in tidal volumes, and/or failure to sigh on a regular basis. Even when they do sigh there is less stretch due to their lower IC. Both could lead to an increase in ASM stiffness and contractility and to atelectasis which is unresolvable with a DI. Also inhibiting vagal tone does not entirely resolve the airway wall/ASM stiffness. Figure 2:Rrs to Rmin traces for each subject group • Healthy subjects had the lowest Rrs and Rmin. When a challenge is administered to a healthy subject their Rrs could be increased to that of a baseline asthmatic, however there is only a minor increase in Rmin. • Asthmatics have a significantly higher Rmin when compared to healthy subjects at baseline and post challenge. • Subjects with SCI have also have an elevated Rrs and Rmin which are both statistically significantly larger than healthy subject. Protocol • Data from 8 healthy pre and post bronchial challenge, and 10 asthmatics pre and post bronchial challenge were acquired from a previous study (2) • New data from 27 SCI (8 Cervical, 13 Thoracic, and 6 Lumbar) subjects has been acquired • Subject is told to take 5 tidal breaths followed by a DI to TLC and then to return to tidal breathing for 5 more breaths • FRC Data was measured via helium dilution * * p<0.05 when compared to healthy at baseline ** p<0.05 based on paired T test Summary N=10 N=5 N=26 N=8 N=13 N=8 * Figure 5 Rminas a function of Rrs,IC, and FEV1 % predicted * * Subject 1 * • Subject groups in which enhanced airway hyperreactivity is reported also show a depressed ability to maximally dilate their airways. • The primary mechanisms controlling maximal dilation is likely a function of maximal elastic recoil pressure and airway smooth muscle stiffness. • Current and past data indicate that in asthma abnormalities in ASM is the primary contributor to hyperreactivity. • In SCI it remains unclear if ASM is abnormal or if increased Rrs is a result of low lung volumes (low FRC and TLC). Future studies should measure elastic recoil pressure during the same maneuvers and also test the reactivity of each subject group explicitly. • The SCI subjects and asthmatic subjects have a similar correlation between Rmin as a function of Rrs and this correlation is markedly different from that of healthy subjects, who seem to have a plateau in Rmin achievable. • The Rmin does not correlate with IC or FEV1. • The FEV1 vs. Rmin data can differentiate cleanly between healthy and asthmatic subjects. ** DI Post Challenge Thoracic SCI Cervical SCI Lumbar SCI Post Chal Baseline Baseline All SCI Subject2 References DI Rmin Figure 3: Rmin for each subject group • A. Jensen, H. Atileh, B. Suki, E. Ingenito, and K. Lutchen. Airway Caliber in Healthy and Asthmatic Subjects: Effects of Bronchial Challenge and Deep Inspiration. J Appl Physiol 2001 96:506-515 • L. Black, R. Dellaca, K. Jung, H. Atileh, E. Israel, E. Ingenito, and K. Lutchen. Tracking Variations in Airway Caliber by Using Total Respiratory Vs. Airway Resistance in Healthy and Asthmatic Subjects. J. Appl Physiol 2003 95:511-518 • E. Singas, M. Lesser, A. Spungen, W. Bauman, and P Almenoff. Airway Hyperresponsiveness to Methacholine in Subjects With Spinal Cord Injury. Chest Oct. 1996 110(4):911-915 • P. Dicpinigaitis, A. Spungen, W. Bauman, A. Absgarten, and P. Almenoff. Bronchial Hyperresponsiveness After Cervical Spinal Cord Injury. Chest April 1994 109(4):1073-1076 • D. Grimm, R. DeLuca, M. Lesser, W. Bauman, and P. Almenoff. Effects of GABA-B Agonist Baclofen on Bronchial Hyperreactivity to Inhaled Histamine in Subjects with Dervical Spinal Cord Injury. Lung 1997 175:333-341 • Healthy subjects have the smallest Rmin value, which becomes slightly increased by bronchial challenge. • Asthmatic Rmin are elevated at baseline and more so after challenge. • Subjects with SCI all have values that are similar to that of baseline asthmatics. If the subject with a Lumbar injury in figure 2, that has a very distinct resistance value from all other SCI subjects is omitted (see * figure 2), then there is evidence of a trend for Rmin to be dependent on injury level. Specifically subjects with cervical SCI have the highest Rmin. Figure 1 Raw data for 2 SCI subjects with thoracic injuries FRC TLC FRC TLC FRC TLC • Both subject 1 and 2 have a similar elevated Rmin (1.75 and 1.6 respectively), however subject 1’s inspiratory capacity is 4 times larger than subject 2’s. Figure 6 FRC %pred. And TLC %pred for subjects with SCI • The decreased FRC values could be partly responsible for the increased Rrs at baseline, possibly even independent of airway tone. The decrease in FRC could be caused by atlectasis, or by increases in lung stiffness. Supported by NIH HLB 62269, the DVA Cooperative Studies Program and NIH R01 HD42141