Download
1 / 16
170 likes | 232 Views
Explore the complexities of prolactin testing through case studies, mechanisms, and prevention methods. Learn about falsely low and falsely high results, including the hook effect and macroprolactin. Understand how dilution testing can prevent misdiagnosis in patients with prolactinomas.

E N D
Prolactin- a good example to discuss laboratory pitfalls • Falsely low • Falsely high • Both are well described
Falsely low results • High dose hook effect • Serum with very large amount of prolactin gives very low result on an immunoassay system. • Other terms: Antigen excess, prozone effect
Case History The patient was a 37-year-old man who developed visual disturbances and was found to have a large infiltrating pituitary adenoma of 5.5 x 4 x 3 cm. Before surgery, 17 serial prolactin measurements in duplicate were determined and showed values from 41 to 48 µg/L (normal, <14 µg/L). The patient had incomplete transsphenoidal resection of his large cystic tumor. Pathological and immunocytochemical studies showed typical characteristics of prolactinoma, where all cells were positive with anti-prolactin serum. Dilution studies done on the patient's serum obtained before surgery showed an initial prolactin level of 31 795 µg/L. After 15 months of treatment with bromocriptine, 2.5 mg thrice daily, the tomographic scan showed a marked decrease in the size of the adenoma, and prolactin levels diminished from 11 171 to 227 µg/L. Comtois R; Robert F; Hardy J Immunoradiometric Assays May Miss High Prolactin Levels Ann Int Med 1993:119 173-4
Case History A 65-year-old man sought medical attention because of headaches, personality changes, and "bulging" eyes. Cranial magnetic resonance imaging disclosed a 10-cm-diameter, lobulated, heterogeneous, locally invasive mass in the anterior skull base and cranial fossa. Initial laboratory testing showed a prolactin level of 164.5 ng/mL (normal range, 1.6 to 18.8). The pathology specimen from his surgical debulking procedure was consistent with prolactinoma. Retesting of the original serum prolactin sample with serial dilutions revealed a prolactin level of 26,000 ng/mL. A postoperative diluted prolactin level was 22,000 ng/mL. Both prolactin samples demonstrated the hook effect. Dopamine agonist therapy was initiated, and the prolactin level and size of the tumor decreased substantially.
Diagnosis and Prevention • Dilution testing can counteract this assay phenomenon. • Clinicians should be aware of this laboratory phenomenon when evaluating large pituitary or parasellar masses. When the hook effect is suspected, dilution testing of prolactin samples may prevent incorrect diagnosis and unnecessary surgical intervention in patients with prolactinomas.
Falsely high results • Patients with high circulating PRL, which is biologically inactive • Not exactly ‘falsely’ high, but the PRL molecule measured has a large size and cannot leave the circulation to exert its action. • Laboratories prefer not to measure them with their routine PRL assay.
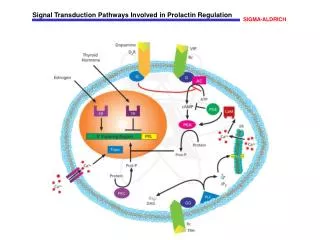
Circulating PRL species in usual patient with hyperprolactinaemia • Monomeric PRL 23 kDa 60-90% • Big PRL 45 – 60 kDa 15-30% • Big-Big PRL >100 kDa 0-10% • = Macroprolactin • Not a definitive single species • PRL bound to IgG (anti-PRL autoantibody) • Complex of covalently or noncovalently bound PRL
Characteristics • Clear slowly • Do not leave circulation, therefore do not exert in vivo action • May have in vitro action • Detectable by immunoassays • Some assays detect them similar to monomeric PRL, while other do not pick them up (epitope concealed by IgG, etc)
Incidence • Around 10% in an endocrine practice • ? More on female, but PRL is more commonly measured in female • Higher percentage in tertiary referal practice • ?more common in autoimmune disease
Case History • The authors report the case of a 37-year-old woman who presented with amenorrhea and an increased level of serum prolactin. Magnetic resonance images of the pituitary revealed a lesion with characteristics consistent with those of a microadenoma. Transsphenoidal exploration was performed, but a prolactinoma was not found. After endocrinological review, the patient's hyperprolactinemia was found to be caused by the presence of macroprolactin and her amenorrhea was due to intense exercise and low body weight. • Cattaneo, FA,Fahie-Wilson MN Concomitant occurrence of macroprolactin, exercise-induced amenorrhea, and a pituitary lesion: a diagnostic pitfall J Neurosurg 2001;95:334-7
Method of detection • Gel filtration chromatography • Not routine • Precipitation with PEG • The macroprolactin precipitates out • Samples with macroprolactin has a significant drop of PRL value after PEG precipitation • Simple, widely acceptable and effective screening test
Fig. 1. Mean serum PRL levels reported by nine different immunoanalyzer user groups in specimens collected from 10 macroprolactinemic subjects. For comparative purposes, the PRL level in each specimen following removal of macroprolactin by gel filtration is shown. From: Smith: J Clin Endocrinol Metab, Volume 87(12).December 2002.5410-5415
Recommendation • Include macroprolactinaemia in the differential diagnosis of hyperprolactinaemia • Use PEG screening method to screen for macroprolactin if there is a clinical suspicion. • For laboratories using method with high cross reactivity to macroprolactin, routine PEG precipitation for any sera with high prolactin is recommended.