Download
1 / 29
300 likes | 704 Views
TUMORS OF THE SALIVARY GLANDS. TUMORS OF THE SALIVARY GLANDS MASSES. DIFFERENTIAL DIAGNOSIS OF A SALIVARY GLAND MASS: INFLAMMATION (PAROTIDITIS) MUMPS CALCULI NEOPLASM. TUMORS OF THE SALIVARY GLANDS. INCIDENCE: 3/100,000 3%ALL BODY TUMORS

E N D
TUMORS OF THE SALIVARY GLANDS MASSES • DIFFERENTIAL DIAGNOSIS OF A SALIVARY GLAND MASS: • INFLAMMATION (PAROTIDITIS) • MUMPS • CALCULI • NEOPLASM
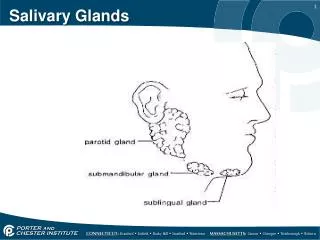
TUMORS OF THE SALIVARY GLANDS • INCIDENCE: 3/100,000 • 3%ALL BODY TUMORS • LOCATION OF SALIVARY GLAND TUMORS: 85% PAROTID, 10% SUBMANDIBULAR, 1% SUBLINGUAL, 4-5% MINOR SALIVARY GLANDS
TUMORS OF THE SALIVARY GLANDS BENIGN MASSES • 80%OF ALL BENIGN LESIONS ARISE IN THE LATERAL (TAIL) OF THE PAROTID GLAND. • SUPERFICIAL PAROTIDECTOMY WITH PRESERVATION OF THE FACIAL NERVE • TOTAL SUBMANDIBULAR AND SUBLINGUAL GLAND RESECTION
TUMORS OF THE SALIVARY GLANDS BENIGN MASSESPLEOMORPHIC ADENOMA • BENIGN MIXED TUMOR • MYOEPITHELIAL AND EPIDERMOID CELL ORIGIN • MOST COMMON NEOPLASM IN THE PAROTID GLAND ACCOUNTS FOR 65% OF ALL OF THE PAROTID TUMORS.
TUMORS OF THE SALIVARY GLANDS BENIGN MASSESPLEOMORPHIC ADENOMA • TREATMENT: WIDE RESECTION OF THE TUMOR • AVOID SHELLING OUT THE LESION • RECURRENCE: PRIMARY DUE TO INADEQUATE RESECTION • LESIONS ARE MORE AGGRESSIVE WHEN THEY RECUR.
TUMORS OF THE SALIVARY GLANDS BENIGN MASSESWARTHIN’S TUMOR (ADENOLYMPHOMA) • SECOND MOST COMMON PAROTID TUMOR • MALE : FEMALE 5 : 1 • BILATERAL 10% • PRIMARILY LOCATED IN THE LATERAL GLAND HOWEVER MULTICENTRICITY IS DESCRIBED. • PEA SOUP BROWN MUCOID MATERIAL ON SECTIONING • TREATMENT: LATERAL OR TOTAL GLANDULAR RESECTION
TUMORS OF THE SALIVARY GLANDS BENIGN MASSESWARTHIN’S TUMOR (ADENOLYMPHOMA) • 90%CURED WITH RESECTION • 10%RECUR DUE TO MULTICENTRICITY OR INADEQUATE RESECTION.
TUMORS OF THE SALIVARY GLANDS BENIGN MASSESONCOCYTOMA • PRINCIPALLY A PAROTID GLAND TUMOR • 5TH DECADE • PROBABLY DUE TO HYPERPLASIA FROM AGING • >1%SALIVARY GLAND TUMORS • CYSTIC COMPONENT HAS BEEN IDENTIFIED.
TUMORS OF THE SALIVARY GLANDS BENIGN MASSESBASAL CELL ADENOMA • COMMON IN THE LATERAL PAROTID AND THE SUBMUCOSAL GLANDS IN THE UPPER LIP. • TREATMENT: LATERAL OR TOTAL GLANDULAR RESECTION.
TUMORS OF THE SALIVARY GLANDS BENIGN MASSESHEMANGIOMA • 50%OF ALL PAROTID TUMORS IN CHILDREN • TREATMENT: ENVOLUTION BY THE AGE OF 5 IS COMMON • CN VII: SUPERFICIAL LOCATION IN CHILDREN THUS OPERATIVE INTERVENTION SHOULD BE AVOIDED AND LET ENVOLUTION PROCEED UNLESS THERE IS UNCONTROLLED BLEEDING. • STEROID THERAPY
TUMORS OF THE SALIVARY GLANDS BENIGN MASSESLIPOMA • 4%OF ALL PAROTID TUMORS • MALE PREDOMINANCE • 4-5%TH DECADE • TREATMENT: LATERAL OR TOTAL GLANDULAR RESECTION
TUMORS OF THE SALIVARY GLANDS BENIGN MASSESMYXOMA • SLOW GROWING • INFILTRATIVE • TREATMENT: WIDE RESECTION OR TOTAL GLANDULAR REMOVAL
TUMORS OF THE SALIVARY GLANDS MALIGNANT MASSES • PROGNOSIS: PALATE > PAROTID > SUBMANDIBULAR / SUBLINGUAL GLAND • 5TH-6TH DECADE • RATE OF GROWTH DOES NOT CORRELATE WITH THE DEGREE OF MALIGNANCY • LUNG/BONE: PRIMARY METASTATIC SITES • PRIOR RADIOTHERAPY INCREASES THE RISK OF A SALIVARY GLAND MALIGNANCY.
TUMORS OF THE SALIVARY GLANDS MALIGNANT MASSESMUCOEPIDERMOID CARCINOMA • MUCOUS AND EPIDERMOID CELL ORIGIN • 6%OF ALL PAROTID TUMORS - MOST COMMON MALIGNANCY • 65%FOUND IN THE PAROTID GLAND • 18%OF ALL MALIGNANT TUMORS OF THE SALIVARY GLANDS
TUMORS OF THE SALIVARY GLANDS MALIGNANT MASSESMUCOEPIDERMOID CARCINOMA • LOW, INTERMEDIATE AND HIGH GRADES • 4-6TH DECADE • 8%CN VII INVOLVEMENT AT THE TIME OF PRESENTATION • 10%LYMPH NODE METASTASIS
TUMORS OF THE SALIVARY GLANDS MALIGNANT MASSESMUCOEPIDERMOID CARCINOMA • TREATMENT: TOTAL GLANDULAR RESECTION +/- NECK NODE DISSECTION • CN VII: SPARE NERVE UNLESS INVOLVED WITH TUMOR. • POSTOPERATIVE RADIOTHERAPY DEPENDING ON MARGINS, EXTRACAPSULAR EXTENSION FROM LYMPH NODES, PERINEURAL INVOLVEMENT, OR INVOLVEMENT OF SURROUNDING STRUCTURES
TUMORS OF THE SALIVARY GLANDS MALIGNANT MASSESMUCOEPIDERMOID CARCINOMA • RECURRENCE RATE 15-25%, USUALLY DUE TO INADEQUATE RESECTION. • WHEN MUCUOEPIDERMOID CARCINOMA IS LOCATED IN THE SUBMANDIBULAR GLAND, THE TUMOR IS MORE AGGRESSIVE. • RARELY INVOLVES THE SUBLINGUAL GLAND
TUMORS OF THE SALIVARY GLANDS MALIGNANT MASSESADENOID CYSTIC CARCINOMA (CYLINDROMA) • MOST COMMON MALIGNANT TUMOR OF THE SUBMANDIBULAR GLANDS AND THE SECOND MOST COMMON PAROTID MALIGNANCY • 25-30%CN VII PARALYSIS/PARESIS ON PRESENTATION • PERINEURAL INVASION IS COMMON • GRAY PINK WITH CRIBRIFORM HISTOLOGY
TUMORS OF THE SALIVARY GLANDS MALIGNANT MASSESADENOID CYSTIC CARCINOMA (CYLINDROMA) • UNPREDICTABLE TUMOR • SLOW GROWING, HOWEVER, RELENTLESS DISEASE • LUNG METASTASIS COMMON • LYMPH NODE INVOLVEMENT NOT COMMON
TUMORS OF THE SALIVARY GLANDS MALIGNANT MASSESADENOID CYSTIC CARCINOMA (CYLINDROMA) • TREATMENT: SURGICAL RESECTION OF THE GLAND WITH POSSIBLE NERVE RESECTION IF INVOLVED • POSTOPERATIVE RADIOTHERAPY
MALIGNANT PLEOMORPHIC ADENOMA (MALIGNANT MIXED TUMOR OR CARCINOMA EX PLEOMORPHIC ADENOMA) • ETIOLOGY: MALIGNANT TRANSFORMATION OF A PLEOMORPHIC ADENOMA • 5-6TH DECADE • AVERAGE DURATION OF THE LESION IS PRESENT 10 YEARS BEFORE BEING DIAGNOSED • TREATMENT: GLANDULAR RESECTION WITH NERVE RESECTION IF INVOLVED WITH TUMOR
ACINOUS (ACINIC) CELL CARCINOMA • LOW, INTERMEDIATE AND HIGH GRADE • INTRAVASCULAR EXTENSION • 3RD-6TH DECADE • METASTASIS TO THE LUNG AND BONE (VERTEBRAE) • TREATMENT: GLANDULAR RESECTION • RADIOTHERAPY IS NOT EFFECTIVE
TUMORS OF THE SALIVARY GLANDS MALIGNANT MASSESSQUAMOUS CELL CARCINOMA • IS IT A METASTATIC LESION? • 1/3HAVE FACIAL NERVE INVOLVEMENT AT THE TIME OF PRESENTATION • MALE > FEMALE • 6TH DECADE • TOTAL GLANDULAR RESECTION • 10YEAR SURVIVAL: 45%
ADENOCARCINOMA • USUALLY FIXED TO THE SURROUNDING STRUCTURES • MALE > FEMALE • 3RD - 6TH DECADE • 22%FACIAL NERVE INVOLVEMENT AT THE TIME OF PRESENTATION • 25%METASTASIS AT THE TIME OF PRESENTATION • GLANDULAR RESECTION WITH NERVE RESECTION IF INVOLVED WITH TUMOR • NECK DISSECTION • POSTOPERATIVE RADIOTHERAPY
TUMORS OF THE SALIVARY GLANDS MALIGNANT MASSESUNDIFFERENTIATED CARCINOMA • 7TH-8TH DECADE • 33%FACIAL NERVE INVOLVEMENT AT THE TIME OF PRESENTATION • HIGHLY MALIGNANT • TREATMENT: GLANDULAR RESECTION, NECK DISSECTION, POSTOPERATIVE RADIOTHERAPY • NERVE RESECTION IF INVOLVED
TUMORS OF THE SALIVARY GLANDS COMPLICATIONS OF SURGICAL INTERVENTION • ORAL FISTULAS • FACIAL NERVE INJURY • LOSS OF EAR SENSATION • FREY’S SYNDROME (GUSTATORY SWEATING) • SKIN NECROSIS