Download
1 / 55
550 likes | 601 Views
Comprehensive update on IPMN, including classification, investigation methods, indications for resection, and follow-up strategies based on international guidelines. Discusses prognosis, surgical techniques, and surveillance protocols.

E N D
Management of intraductal papillary mucinous neoplasm of pancreas (IPMN)An Update KOK SIU YAN AMY United Christian Hospital
IPMN • Introduction • Classification • Investigation • Indication for resection • Methods of resection • Follow-up • Prognosis
Introduction • History: 1982 • Described by Ohashi and his colleagues • Incidence ~2.04 per 100 000 • Autopsy studies 25% of cystic pancreatic lesions • 30-50% may become invasive • Accounts for 5-7% of all pancreatic neoplasm Dtsch Arztebl Int. 2011 Nov;108(46):788-94. Intraductal papillary mucinous neoplasia (IPMN) of the pancreas: its diagnosis, treatment, and prognosis. Grützmann R, Post S, Saeger HD, Niedergethmann
Presentation DtschArztebl Int. 2011 Nov;108(46):788-94.. Intraductal papillary mucinousneoplasia (IPMN) of the pancreas: its diagnosis, treatment, and prognosis. Grützmann R, Post S, Saeger HD, Niedergethmann M.
Management guideline First international consensus guideline in 2006 and was revised in 2012
classification • Main duct • Branch duct • Mixed
Investigation • USG • CT • MRI + MRCP • EUS +/- FNAC • ERCP • Intraductal USG or pancreatoscopy
investigation • USG • Size and extent • CT • Diffusely distended pancreatic duct with mucinous filling defects and cystic space occupying lesions • Sensitivity 42%
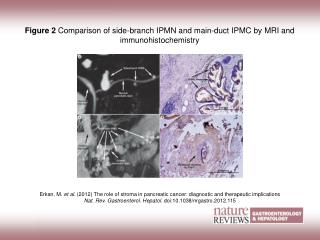
investigation • MRI with MRCP • Entire pancreatic parenchyma and the intra-abdominal organs • More sensitive to detect mural nodules • Sensitivity 88% Br J Surg. 2009 Jan;96(1):5-20. Preoperative tissue diagnosis for tumours of the pancreas. Hartwig W, Schneider L, Diener MK, Bergmann F, Büchler MW, Werner J.
Investigation • EUS-FNA • CEA • Amylase • Cytology • Molecular analysis • Investigational • Small BD-IPMN
INDICATIONS FOR RESECTION • MD-IPMN • BD-IPMN
2006 guideline: MD-IPMN • Main duct dilatation≥1cm • Frequency of malignancy: 60-92% • No clinical parameters accurately discriminate malignant and non-malignant lesion RESECT ALL MAIN DUCT AND MIXED VARIANT IPMN IF SURGICALLY FIT
2012 guideline: BD-IPMN • High-risk stigmata • Obstructive jaundice in patient with cystic lesion of the head of pancreas • Enhancing solid component within cyst • Main pancreatic duct ≥10mm in size CONSIDER SURGERY IF CLINICALLY APPROPRIATE
2012 guideline: BD-IPMN • Worrisome features • Clinical: pancreatitis • Imaging: • cyst≥3cm • Thickened/enhancing cyst walls • Main duct size 5-9mm • Non-enhancing mural nodule • Abrupt change in calibre of pancreatic duct with distal pancreatic atrophy PERFORM ENDOSCOPIC ULTRASOUND
2012 guideline: BD-IPMN • EUS features: • Definite mural nodule • Main duct features suspicious for involvement • Cytology: suspicious or positive for malignancy CONSIDER SURGERY IF CLINICALLY APPROPRIATE
2012 guideline: MD-IPMN • MD-IPMN • Main duct dilatation≥5mm • 5-9mm worrisom features • Evaluation • No immediate resection
Method of pancreatectomy • According to site and extend of disease • Pancreatoduodenectomy • Distal pancreatectomy • Total pancreatectomy • Limited resection • Excision • Enucleation • Uncinatectomy • Laparoscopy +/- lymph node dissection
follow-up • Non-resected IPMN • Surgically resected IPMN
2006: resected IPMN • Benign: • Yearly CT/MRI • Malignant • 6 monthly CT/MRI • CEA & CA19.9 no value
2012: Resected IPMN • Surgical margin status • normal pancreatic tissue • non-dysplastic changes • low grade dysplasia • moderate grade dysplasia • invasive carcinoma Repeat exam 2-5 years Hx/PE/MRCP half-yearly Identical to PDAC
prognosis • Complete resection of noninvasive IPMN • 5 year survival rate 95% • Complete resection of early stage tumors(T1N0) • 5 year survival rate 60% • Advanced or nodal positive tumors • 5 year survival rate 36%
investigation • High-risk stigmata surgery • Smaller cyst + worrisome features EUS • Cyst >3cm + NO worrisome features EUS if elderly • Cyst ≤3cm + NO worrisome features surveillance
Md-ipmn • High incidence of malignant/invasive lesions (61.6%/43.1%) • Segmental ectatic type/Diffuse type with focal lesions • Diffuse type without focal lesions • Frozen section • Intraductal USG/pancreatoscopy
Bd-ipmn • Mean frequency of malignancy/invasive cancer (25.5/17.7%) • Elderly • Annual malignancy risk 2-3% • High risk factors: • Mural nodules • High grade dysplasia/Positive cytology • Rapidly increasing size • Individual decision
Family history • One 1st degree relative with PDAC 2.3-fold increased risk • high-quality MRI/MRCP or CT and EUS • Malignant stigmata/worrisome features • resection • No malignant stigmata/worrisome features • MRI/MRCP or CT at 3-month intervals • EUS annually for first 2 years
Distinction of BD-IPMN from mcn & other pancreatic cyst • Combination of clinical & imaging characteristics can provide preoperative diagnosis of cyst type • Multidetector CT (MDCT) & MRCP are useful for defining morphology, location, multiplicity, and communication with the MPD • Distinguishing features: multiplicity & visualisation of a connection to MPD • EUS: delineate malignant characteristics eg mural nodules & invasion but operator dependent • Cyst fluid x CEA, amylase & cytology cannot distinguish MCN & IPMN • Molecular analysis for GNAS mutations can distinguish MCN from BD-IPMN
Distinction of BD-IPMN from serous cystic neoplasm (SCN) • 3 morphological patterns: • Polycystic • Honeycomb • Oligocystic Distinguished from SCN with a polycystic or honeycomb pattern by CT or MRCP Differentiation between a small oligocystic SCN & a BD-IPMN may require EUS-FNA with cyst fluid CEA determination
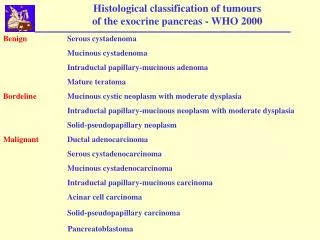
Pancreatic cyst • Neoplastic cysts: • Non-mucinous • Serous cystic neoplasm (SCN) • Solid pseudopapillary neoplasm (SPN) • Mucinous • Mucinous cystic neoplasm (MCN) • Intraductal papillary mucinous neoplasm (IPMN)
MCN • Low prevalence of invasive carcinoma (<15%) • Resection is recommended • Young • Risk of progression • Locations in body and tail • High cost of long-term FU • Distal pancreatectomy • Parenchymal-sparing resection (middle pancreatectomy) • Laparoscopic
EUS-FNA • Apart from imaging, elevated cyst fluid CEA is a marker that distinguishes mucinous from non mucinous cysts, but NOT benign from malignant cysts • A cut off of >/=192-200ng/ml is ~80% accurate for diagnosis of mucinous cyst • Cyst fluid amylase is shown to be not uniformly elevated in IPMN • Fluid cytology may add value especially for evaluation of a small BD-IPMN without “worrisome features”. • High grade epithelial atypia recognised in cyst fluid predicted malignancy in a mucinous cyst with 72% sensitivity in one study and detected 30% more cancers in small IPMN without worrisome features in another study • Some studies showed molecular analysis of cyst fluid may be helpful in distinguishing significant mucinous cysts from indolent cysts that can be conservatively managed • However, in view of the inconclusive evidence, this guideline suggests cyst fluid analysis is still investigational, but is recommended for evaluation of small BD-IPMN without worrisome features only in centres with expertise in EUS-FNA and cytological interpretation
prognosis • Synchronous/metachronous malignant diseases in extra-pancreatic organs • 20-30% • Frequency and location of extra-pancreatic malignancies differs • GI cancer is common in Asia • Skin/breast/prostatic cancers common in US
conclusion • This comprehensive guideline has lowered the criterion for characterising MD-IPMN to MPD dilatation of >5mm without losing specificity for radiologic diagnosis • -high risk stigmata and worrisome features have been defined to stratify risk of malignancy in BD-IPMN and consider resection or increased freq of surveillance • -resection is recommended for all surgically fit patients with MD-IPMN or MCN • Indications for resection of BD-IPMN are more conservative • BD IPMN >3cm without high risk stigmata can be observed without immediate resection
A previous history of diabetes, especially with insulin use, CP, and family history of PDAC are all relevant risk factors for the development of IPMN. • Am J Gastroenterol. 2013 Jun;108(6):1003-9. doi: 10.1038/ajg.2013.42. Epub 2013 Mar 5. • Risk factors for intraductal papillary mucinous neoplasm (IPMN) of the pancreas: a multicentre case-control study.
MR LKF 75/m • Good past health • No history of pancreatitis • No family history of pancreatic cancer • Physical examination: unremarkable
Ultrasound 2.5cm cystic lesion over pancreas What should we do next?
Pancreatic cyst Differential diagnosis • Benign – Pseudocyst – Serous cystic neoplasm (SCN) – Simple cyst, retention cyst, congential, lymphoepithelial cyst • Potentially malignant – Intraductal papillary mucinous neoplasm (IPMN) – Mucinous cystic neoplasm (MCN) – Solid pseudopapillary neoplasm (SPN) – Neuroendocrine tumor • Malignant – Ductal adenocarcinoma
Pancreatic cyst Pathological diagnosis (n = 212) Fernandez-del Castillo et al. Arch Surg 2003
introduction • WHO classification of digestive system 2010 • IPMN with low or intermediate grade dysplasia • IPMN with high grade dysplasia • IPMN with invasive cancer