Download
1 / 66
700 likes | 745 Views
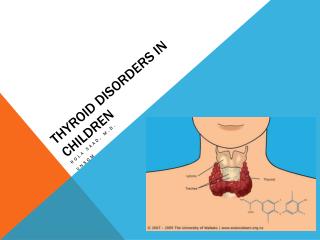
Common Thyroid Disorders in Children. Dr Sarar Mohamed FRCPCH (UK), MRCP (UK), CCST (Ire), CPT (Ire), DCH (Ire), MD Consultant Paediatric Endocrinologist & Metabolist Assistant Professor of Pediatrics King Saud University. Endocrine Glands. Agenda. Thyroid Anatomy and physiology

E N D
. Common Thyroid Disorders in Children Dr Sarar Mohamed FRCPCH (UK), MRCP (UK), CCST (Ire), CPT (Ire), DCH (Ire), MD Consultant Paediatric Endocrinologist & Metabolist Assistant Professor of Pediatrics King Saud University
. Agenda • Thyroid Anatomy and physiology • Thyroid Function Test • Congenital Hypothyroidism • Newborn screening for congenital hypothyroidism • Acquired hypothyroidism • Hyperthyroidism • Causes of goitre
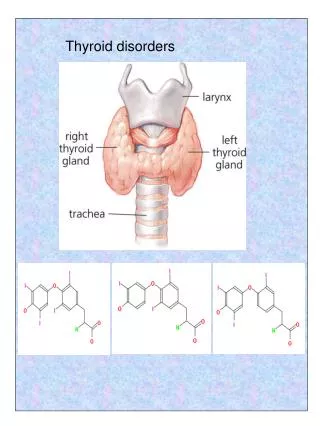
THYROID GLAND Location: Located close to thyroid cartilage. Has two lateral lobes connected by thyroid isthmus medially. Development: first endocrine gland to appear during development. Develops from endodermal floor of early pharynx
THYROID GLAND Innervation: Vagus Nerve (X) Arterial Supply: superior thyroid artery (branch of external carotid artery). Functions: THYROXIN –regulate rate of metabolism CALCITONIN –decreases levels of calcium and phosphate in the blood (partially antagonistic to parathyroid hormone).
Production of Thyroid Hormones NIS (Na+/I- Sympoter) TPO
t1/2 = 5-7d t1/2 = < 24 hrs
Normal Daily Thyroid Secretion Rate: T4 = 100 ug/day T3 = 6 ug/day ( ratio T4:T3 = 14:1 ) T4 Protein binding+ 0.03% free T4 85% (peripheral conversion) T3 Protein binding +0.3% free T3 15% (10-20x less than T4)
Thyroid Function: blood tests TSH 0.4 –5.0 mU/L Free T4 (thyroxine) 9.1 – 23.8 pM Free T3 (triiodothyronine) 2.23-5.3 pM
Effects of thyroid hormones • Fetal brain & skeletal maturation • Increase in basal metabolic rate • Inotropic & chronotropic effects on heart • Stimulates gut motility • Increase bone turnover • Increase in serum glucose, decrease in serum cholesterol • Play role in thermal regulation
Dysfunction Thyroid Gland 1. Too little thyroxin – hypothyroidism a. short stature (aquiered), developmental delay (congenital) 2. Too much thyroxin – hyperthyroidism a. Agitation, irritability, & weight loss
Hypothyroidism • Decreased thyroid hormone levels • Low T4 • Possibly Low T3 too. • Raised TSH (unless pituitary problem!)
. Causes of hypothyroidism • Congenital • Autoimmune (Hashimoto) • Iodine deficiency • Subacute thyroiditis • Drugs (amiodarone) • Irradiation • Thyroid surgery • Central hypothyroidism (radiotherapy, surgery, tumor)
. Clinical features of Acquired hypothyroidism • Weight gain • Goitre • Short sature • Fatigue • Constipation • Dry skin • Cold Intolerance • Hoarseness • Sinus Bradycardia
. Diagnosis • High TSH, low T4 • Thyroid antibodies
Hashimoto’s Disease • Most common cause of hypothyroidism • Autoimmune lymphocytic thyroiditis • Antithyroid antibodies: • Thyroglobulin Ab • Microsomal Ab • TSH-R Ab (block) • Females > Males • Runs in Families!
Subacute (de Quervain’s) Thyroiditis • Preceding viral infection • Infiltration of the gland with granulomas • Painful goitre • Hyperthyroid phase Hypothyroid phase
Treatment of Hypothyroidism • Replacement thyroid hormone medication: Thyroxine
. Congenital Hypothyroidism: Causes • Agenesis or dysgenesis of thyroid gland • Dyshormonogenesis • Ectopic gland • Maternal hypothyroidism
Newborn Screening Facts Normal Newborn Immature Hypothalamic Pituitary Thyroid Axis Mother supplies T4 to fetus via placenta Mother Fetus T4 Mid-Gestation T4 Mature Hypothalamic Pituitary Thyroid Axis Euthyroid Mother Pregnancy
Newborn Screening Clinical Features of Congenital Hypothyroidism
Newborn Screening Congenital Hypothyroidism X suspect Clinical Biochemical (screening) Confirm Lab ( TSH & FT4 ) Optional • T scan • B age Rx & FU Thyroxine Growth & D TSH & FT4
Newborn Screening Management Primary Congenital Hypothyroidism High TSH & Low T4 Thyroxine Dose Form Goals 10 -15 ug/kg/day 12 -17 ug/kg/day 37.5 – 50 ug/day Higher dose in Severe cases T4< 5ug/dl Tablets 25-50-75 ug Crush it, add to 5-10 cc water Or milk Normal T4 In 2 wks (upper ½ of N) Normal TSH In one month (lower ½ of N)
Newborn Screening • Definitions • Screening: search for a disease in a large unselected population • PKU • Congenital hypothyroidism
Newborn Screening Principal of newborn screening • Aim is to identify affected infants before development of clinical signs
Newborn Screening Success Stories in Pediatric Medicine • Immunization programs • Newborn Screening program • Oral Rehydration Therapy • Pencillin
Newborn Screening Phenylketonuria Guthrie Test 1962, Robert Guthrie
Glucose-6-phosphate dehydrogenase deficiency (G6PD) Sickle cell anemia (Hb SS) > 1 in 5,000; among African-Americans 1 in 400 Sickle-cell disease (Hb S/C) > 1 in 25,000 Hb S/Beta-Thalassemia (Hb S/Th) > 1 in 50,000 Tyrosinemia I (TYR I) < 1 in 100,000 Tyrosinemia II Argininemia Argininosuccinic aciduria (ASA) < 1 in 100,000 Citrullinemia (CIT) < 1 in 100,000 Phenylketonuria (PKU) > 1 in 25,000 Maple syrup urine disease (MSUD) < 1 in 100,000 Homocystinuria (HCY) < 1 in 100,000 Glutaric acidemia type I (GA I) > 1 in 75,000 Glutaric acidemia type II HHH syndrome (Hyperammonemia, hyperornithinemia, homocitrullinuria syndrome) Hydroxymethylglutaryl lyase deficiency (HMG) < 1 in 100,000 Isovaleric acidemia (IVA) < 1 in 100,000 Isobutyryl-CoA dehydrogenase deficiency 2-Methylbutyryl-CoA dehydrogenase deficiency 3-Methylcrotonyl-CoA carboxylase deficiency > 1 in 75,000 Beta-methyl crotonyl carboxylase deficiency 3-Methylglutaconyl-CoA hydratase deficiency Methylmalonyl-CoA mutase deficiency (MUT) > 1 in 75,000 Methylmalonic aciduria, < 1 in 100,000 Beta-ketothiolase deficiency (BKT) < 1 in 100,000 Propionic acidemia (PROP) > 1 in 75,000 Adenosylcobalamin synthesis defects Multiple-CoA carboxylase deficiency (MCD) < 1 in 100,000 Carnitine palmityl transferase deficiency type 2 (CPT) Long-chain acyl-CoA dehydrogenase deficiency (LCAD) Long-chain hydroxyacyl-CoA dehydrogenase deficiency (LCHAD) > 1 in 75,000 Short-chain acyl-CoA dehydrogenase deficiency (SCAD) Short-chain hydroxy Acyl-CoA dehydrogenase deficiency (SCHAD) Medium-chain acyl-CoA dehydrogenase deficiency (MCAD) > 1 in 25,000 Very-long-chain acyl-CoA dehydrogenase deficiency (VLCAD) > 1 in 75,000 Carnitine/acylcarnitine Translocase Deficiency (Translocase) Multiple acyl-CoA dehydrogenase deficiency (MADD) Trifunctional protein deficiency (TFP) < 1 in 100,000 Carnitine uptake defect (CUD) < 1 in 100,000 Congenital toxoplasmosis HIV Cystic fibrosis (CF) > 1 in 5,000 Maternal vitamin B12 deficiency Congenital hypothyroidism (CH) > 1 in 4,000 Biotinidase deficiency (BIOT) > 1 in 75,000 Congenital adrenal hyperplasia (CAH) > 1 in 25,000 Classical galactosemia (GALT) > 1 in 50,000 Newborn Screening Possible screening tests
Newborn Screening Congenital Hypothyroid • Screening started 1974 in Quebec & Pittsburgh • Objective : Eradication of MR secondary to CH • Incidence 1:3000 – 4000 ( more than PKU ) • Female : Male is 2 : 1
Newborn Screening Congenital Hypothyroidism • One of the most common Treatable causes of MR • CH Screening is the most cost effective program • Almost all affected NB have no S/S at birth • Congenital Anomalies increased by 10%(cardiac) • In more than 90% of the cases it is permanent • The earlier dx the better IQ
Wilson Criteria Incidence >1/100,000 Significant morbidity/mortality Successful treatment Reasonable cost Test: specific/sensitive/acceptable Congenital hypothyroidism 1/3,000 to 1/4,000 Mental retardation Thyroxine $3.00 immunoassay Newborn Screening Newborn Screening Criteria
Newborn Screening Screening Technique • Specimen is a blood spot in a filter paper • Obtained by heel brick • Or cord blood
Newborn Screening Good Specimen
. Congenital Hypothyroidism Objective from screening: Eradication of MR secondary to CH Every Newborn is considered Hypothyroid Until Proven Otherwise
Newborn Screening Method & Timing of Thyroid Screening Primary-TSH Backup-T4 Both TSH&T4 Primary-T4 Backup-TSH Venous Blood Cord Blood Age At Birth Age 2-5 days
Newborn Screening Clinical Outcome • Pre-screening data: • Mean IQ = 76
Newborn Screening Clinical Outcome • Post-screening data: • Children screened & treated by age 25 days • Mean IQ = 104
Newborn Screening > screening < screening
Newborn Screening X Congenital Hypothyroidism