Download
1 / 98
1.03k likes | 1.4k Views
Thyroid Disorders. T₃: Triiodothyronine T₄: Thyroxine. I. Hyperthyroidism ( Thyrotoxicosis ). Characterized by hypermetabolism of all body systems & increased serum levels of free thyroid hormones. More common in women. Rare in children Less common than hypothyroidism.

E N D
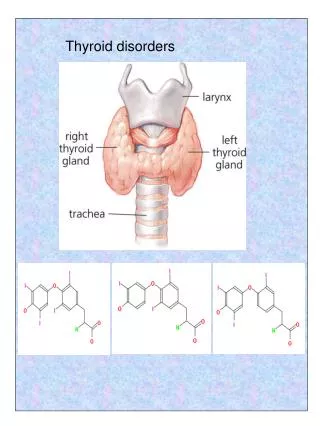
Thyroid Disorders T₃: Triiodothyronine T₄: Thyroxine
I. Hyperthyroidism (Thyrotoxicosis) • Characterized by hypermetabolism of all body systems & increased serum levels of free thyroid hormones. • More common in women. • Rare in children • Less common than hypothyroidism
Thyroid Storm: • Exaggerated form of hypertoxicosis. • Medical emergencyPrompt treatment • May be precipitated by : -Infection -Trauma - Surgery -Embolism -Diabetic ketoacidosis -Others…
Subclinical Hyperthyroidism: • Suppressed TSH level w/ NL thyroid hormone levels. • Symptoms are NOT always present esp. in elderly. • Pathophysiology: See p. 987-990
Treatment Goals of Hyperthyroidism: • Reverse S/S, normalize thyroid hormone levels, min. deleterious S/Es of T₄ on organ systems, prevent thyroid storm, & improve overall functional capacity. • Reverse hyperthyroid complaints. • Reverse hyperthyroid physical findings. • Normalize free T₄, T₃, & TSH levels. • Reduce goiter size.
Improve cardiac function & prevent systemic embolism. 7) Preserve bone density& prevent osteoporosis. 8) Improve emotional well being& quality of life. 9) Support placenta development & maintenance of pregnancy. 10) Promote normal growth, & physical & mental development.
Causes of Hyperthyroidism: (table38.3 p.993) • Graves disease: -Autoimmune -May occur w/ other autoimmune disorders. -Most common cause -Charact. by hyperthyroid. & one or more of the following: * Goiter * Exophthalmos * Dermopathy
2) Toxic Nodules: -Single & multinodular -Autonomous: independent of TSH control. -May be caused by: *Iodine deficiency *Genetic abnormality *Immune System
3) SubacuteThyroiditis: - Inflammatory thyroiditis, i.e.Postpartum(PPT), viral (i.e. de Quervain). - Hyperthyroid. from leakage of thyroid hormones into circulation due to inflamed gland & NOT increased synthesis. -Hypothyroidism may follow.
4) Drug Induced: -Iodides (Jod-Basedow), Amiodarone, Lithium, Cytokines 5) Neonatal thyrotoxicosis (Graves): -Transplacental passage of TRab causing the infant to be extremely ill w/in delivery hrs. -Self-limiting.
6) Hashitoxicosis: -Hyperthyroid phase of Hashimoto thyroiditis 7) T₃ toxicosis: -Preferential secretion of T₃, often precedes T₄ toxicosis. 8) Tumors: -Secretion of thyroid stimulating substances. 9) Factitious: -Self-administration of levothyroxine
Clinical Presentation & Diagnosis: - Characteristics of Graves Dz. p.997 Table 38.6 -SxS of Hyperthyroidism & Hypothyroidism p.995 Table 38.4 - Thyroid Function Tests (TFTs) p.987-988
Diagnosis of Hyperthyroidism : • Confirmed w/ abnormally high levels of FT₄ or TT₃ & undetectable TSH. 2) +Antibodies, opthalmopathy, or dermopathy confirms the diagnosis of Graves. 3) RAIU in Graves but is NOT cost-effective 4) TT₃ & + TRab are essential for atypical presentation, i.e. in elderly.
5) SubacuteThyroiditis (PPT,…), Diagnosis is confirmed by: *Low or undetectable RAIU. * TH levels. *Suppressed or undetectable TSH level. * ESR * No Thyroid Ab. * Leukocytosis, gland tenderness, & S/S of hyper or hypothyroidism.
Therapeutic Plan: (table 38.7, p.998-999) • Major Modalities for Management of Hyperthyroidism, include: 1) Thioamides 2) RAI 3) Surgery ** Treatment must be individualized, each has advantages & limitations **Effective Treatment Selection p.1000, Fig.38.3
Treatment Adjuncts: • Iodides • Iodinated Contrast Media • K Perchlorate • Adrenergic Antagonists • Corticosteroids • Cholestyramine • Rarely Li
In U.S., RAI is most commonly used except in younger pts. for whom Thioamides are used. • In Europe & Japan, Thioamides are the TOC. • Surgery is the last choice unless there is: *Obstructive symptoms or* Malignancy
Treatment is individualized a/c to: 1. Etiology 2. Pt. age 3. Goiter size 4. Thyroid & Medical complications 5. Social & Economic issues
Graves: All 3 methods are effective but pt. or Dr. may prefer meds. over RAI or surgery. • TMG: RAI or surgery > effective than meds., but factors as medical condition or pt. or Dr. may prefer RAI use over surgery. 3.Transient Treatment : may be used when the disease is self-limited, i.e.: * SubacuteThyroiditis (PPT,…) *Neonatal Graves *Drug-Induced Hyperthroidism
In Uncomplicated Graves esp. in children, Thioamidesare preferred until remission. • Thioamides: - Do NOT destroy the gland - Control the disease - Chronic thyroid replacement may not be necessary (not like w/ RAI or Surg.), however, hypothyroid. may still develop eventually.
If RAI or Surgery is selected, most older pts. & all severely ill thyrotoxic pts. should be pretreated w/ Thioamides. • Pretreatment: • Depletes gland of stored hormones. • Hypermetabolic rate. • Prevents leakage of hormone from gland after RAI or during surgery preventing thyroid storm.
Optimal Tx of hyperthyroidism in Graves opthalmopathy is unresolved. • Some prefer RAI or surgery (<desirable) to remove the antigen source (gland) & > effective than thioamides to prevent progressive opthalmopathy. • Prophylactic systemic corticosteroid (e.g., Prednisone 30-40mg daily starting within a few days of RAI & cont. for ~2-3 wks. to prevent further progression of opthalmopathy in pts. w/ re-existing cases. • Hypothyroidism can aggravate preexisting eye complaints. • Hyperthyroidism control & hypothyroidism prevention are essential to prevent progression of opthalmopathy.
Single or Toxic multinodular Dz.: • Best managed with definitive Tx, i.e. RAI or surgery, because spontaneous remission is unlikely. • Hyperthyroid Children: The usual Tx choices are Thioamides & subtotal thyroidectomy, although all 3 methods have been used.
In Pregnancy: • Hyperthyroidism is difficult to manage. • Spontaneous remission may occur because of the decrease in TRab. • Antithyroid meds. are often NOT necessary. • If untreated, complications may occur. • RAI & Iodides are Contraindicated in pregnancy. • Surgery in 2nd trimester is an option.
Neonatal Graves: • Infants extremely ill w/in delivery hrs. • Supportive measures, i.e. *sedation *O₂ *Fluids/Electrolytes • Short-term (temporary) thioamides, iodides, or beta blockers since it is self-limiting. • Symptoms disappear in 1-2 months, therefore, withdraw antithyroids at this time.
SubacuteThyroiditis: • Self-limiting (common spontaneous recovery). • Symptomatic treatment: *Heat *Rest *NSAIDs *Beta-blockers * Thioamides are NOT effective since it is due to thyroid hormone leakage & NOT increase in TH synthesis.
Cont. SubacuteThyroiditis: • Corticosteroids are indicated for severe inflammation if NSAIDs are ineffective. • In Hypothyroid phase: Transient thyroid replacement is used to suppress further TSH stimulation to damaged gland & treat hypothyroid symptoms.
Treatment: Fig.38.3 p.1000 • Pharmacotherapy: • Thioamides: *Long-term 1⁰ therapy for Graves esp. in children & adolescents. *Transiently used to reduce TH levels before definitive therapy w/ RAI or surgery. *TOC for small goiters & mild dz. For whom a high remission rate is likely.
Advantages: • Potential for remission without gland damage. • Limitations: 1.Non-adherence 2.Strict parental & physician supervision in kids. 3.Low success rates. 4. Risk of ADRs.
Thioamides: 1. Methimazole 2. Propylthiouracil (PTU) • They prevent TH synthesis. • PTU (Not Methimazole) inhibits peripheral deiodination of T₄ to T₃. • They suppress TSH receptor Ab level by unknown immunosuppressive MOA.
Thioamides Selection: • Pharmacologic Differences: ** Methimazole is preferred over PTU, because: 1. Single daily dose ( PTU Q6-8H) 2. More potent than PTU 3. Less toxic than PTU @ low doses. 4. Less costly. ** Both are equally effective @ equipotent doses.
PTU is preferred over methimazole in pts. w/ **Thyroid Storm Or **Severe Hyperthyroidism Because: • PTU blocks the conversion of T₄ to T₃ peripherally. • PTU may have faster OA. *PTU is preferred in pregnancy because methimazole may be associated w/ congenital skin defect ( NOT sufficiently supported & has been used in pregnancy without deleterious effects). *Both can be used safely in pregnancy *PTU is preferred in lactation because insignificant amounts are secreted in the breast milk. *Generally,Methimazole is the thioamide of choice EXCEPT in the situations mentioned above where PTU is preferred , or if the patient cannot tolerate methimazole.
No IV preparations of thioamides. • It usually takes 6-8wks before SxS subside & TH normalize. • Initial dose: Methimazole 30-40 mg/d orally or PTU 300-400mg/d in 3-4 divided doses. Tapering down dose only after SxS subside: **Initial dose is reduced gradually by 1/3 each month until daily M.D. of 5-15mg methimazole or 50-150mg PTU is reached.
Baseline FT₄ & WBC count w/ differ. should be done before thioamides are started because agranulocytosis can be induced by thioamides & also hyperthyroidism is associated w/ relative reduction of neutrophils. • FT₄ or FT₄I & TSH should be monitored routinely @ 4-8 wks after starting Tx & after any dose change. • Once stable thioamide M.D. is reached, TFTs should be monitored Q 2-4 or Q3-6 months.
Recommended duration of Tx for Graves is emperic: Generally 12-18 months. • 12 months is the minimum Tx duration recommended to maximize remission potential. • Longer durations can be used if NO ADRs. • Some pts. remain in remission & others relapse ????
Toxic Reactions: • PruriticMaculopapular Skin Rash: Most common & treated w/ antihistamines. • Hepatatis: *If LFTs normalize w/in 3 months of dose reduction, NO need to discontinue PTU. *If there is clinical evidence of hepatitis, D/C PTU immediately. * Routine monitoring of LFTs is required for: 1. Pts. w/ liver dz. history. 2. Hepatitis risk factors, i.e. alcoholism