Download
1 / 30
300 likes | 377 Views
Water and HIV/AIDS. Dr. Kate Tulenko WSP February 20, 2007. Purpose. To make WSP staff familiar with common HIV/AIDS concepts and terminology so they can “talk shop” with health specialists.

E N D
Water and HIV/AIDS Dr. Kate Tulenko WSP February 20, 2007
Purpose • To make WSP staff familiar with common HIV/AIDS concepts and terminology so they can “talk shop” with health specialists. • Train WSP staff to give assistance to MOWs and water utilities to design HIV/AIDS programs for their staff and clients. • Train WSP staff to start a dialogue with MOWs on the health benefits of providing improved WSH to PLWHAs and the need for programs and research.
Outline • Overview of the Human Immunodeficiency Virus • Overview of the HIV/AIDS Pandemic • HIV/AIDS, MOWs, & Water Utilities • Role of WSH in Improving the Lives of PLWHA
HIV Virus • Believed to be a zoonosis (transmitted from animals) • Found in almost all body fluids • Virus: Cannot replicate outside of a living cell • Enters and damages white blood cells, especially helper T cells (CD4)
Transmission • Unprotected Sex • Maternal to Child Transmission • During pregnancy • Breastfeeding • Sharing of Needles • Blood Transfusions
Risk Factors • STDs • Multiple partners • Partner with a risk factors • Use of alcohol and drugs • Lack of power within the relationship • Women, age
Diagnosis • Rapid diagnosis kits and now the gold standard • Detect HIV proteins • Acquired-Immune Deficiency Syndrome • Low CD4 count • Opportunistic infections • TB • Rare cancers • Rare pneumonias • Overwhelming fungal infections (Candida)
Natural History • Time from infection to significant symptoms (Opportunistic Infections) 5 to 10 years • Time from significant symptoms to death: 3 to 5 years if untreated • AIDS in Africa dominated by “Slim Disease”: chronic diarrhea and weight loss
Weakened Immune System • Opportunistic infections (harmless to normal immune system) • Candida • Pneumocystis • Toxoplasmosis • CMV • Lowered infectious doses for standard pathogens
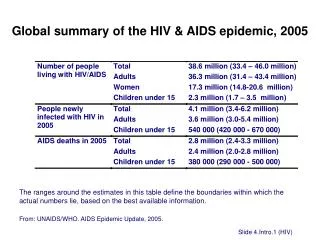
2006 AIDS Statistics • 39 million people infected in the world • 24.7 million in Sub-Saharan Africa • 7.8 million in South East Asia • 2.2 million in Europe and North America • 1.7 million in Latin America • 4.3 million new infections in 2006 • 2.9 million HIV/AIDS related deaths in 2006 • Estimated that around 2million people are receiving ARVs in developing countries
Stages in the Epidemic • Focal: in high risk groups • Commercial sex workers and their clients • Men who have sex with men (MSM) • IV Drug Users (IVDU) • Other high risk occupations: truck drivers, miners, migrant workers • Generalized • General population
Responses • Target messages to high risk groups • Reduce high risk behaviors • Mitigate risk • Counseling and testing • General population • Awareness • Reduction of stigma
TB and Malaria • The AIDS epidemic caused a surge in the TB epidemic • Most PLWHA should be on medication to prevent TB • Hygiene issues associated with TB • People with low grade malaria infections are much more likely to get HIV when exposed • Water issues associated with breeding sites for malaria transmitting mosquitoes
Mitigating Risk • Reduction in number of sexual partners • Decrease in age of first sex • Increase in condom use • Needle cleaning or needle exchange • Male circumcision • Rapid treatment of STDs • Switch infant formula only if it is AFASS. In most low resource settings, HIV+ women should breastfeed • Changes in societal attitudes
The Scourge of Stigma • Prevents people from seeking diagnosis and care • Dying vs Dying from AIDS • In Uganda, the CDC Safe Water System became identified with HIV/AIDS • Use readily available WASH methods
Life with ART Depends on the Quality of Care • Goal: to maximize functional years and delay resistance • Delay ART treatment as long as possible • Criteria • White blood cell count (CD4) • Viral loads • Symptoms • Resistance (what drugs to start on) • Compliance • Monitor • The above plus liver enzymes
Why is it so Difficult to Treat HIV/AIDS? • The virus is protected within cells. • HIV attacks the immune system, the systems that is responsible to eliminating infections. • HIV reproduces rapidly and mutates rapidly. A recipe for drug resistance. • Drugs have to be taken frequently and regularly • Drugs have to be taken for the rest of the patient’s life. • Drugs need to be adjusted for resistance. • Resistance and blood cell count levels, and viral load levels need to be monitored.
Why is it so Difficult to Treat HIV/AIDS? • The drugs have side effects • In addition of ARVs, drugs need to be take to prevent Opportunistic Infections (IOs) • Most PLWHA do not know they are infected. • Even those who know they are infected refuse treatment do to stigma. • HART requires a team of highly trained clinicians and support staff, a strong laboratory system, a good drug stocking. • To prevent resistance, patients usually need to be on three ARVs
Major HIV/AIDS Initiatives • World Bank MAP (Multi-Country AIDS Program): prevention, community based funding, required non-health sectors to be involved • Global Fund: Little technical assistance provided • PEPFAR (USAID): ARV therapy, Prevention of Mother to Child Transmission (PMCT) • WHO 3x5: ARV therapy • Clinton Foundation: ARV therapy
What We Do Know • Improved water can reduce the number and severity of episodes of diarrhea of PLWHA (Increases functional days) • Improved WASH eases the family caregiving burden, especially at the end of life • Issues of disposal of large quantities of HIV infected diarrhea • Infant formula made with improved water can eliminate transmission from breast feeding but ACCESS TO IMPROVED WATER AND FORUMLA MUST BE GUARENTEED FOR AT LEAST 6 MONTHS!! (AFASS)
Key Entry Point: Priority Clients • Higher priority to provide WASH services to symptomatic non-treated PLWHA
Key Entry Point • Mothers and Infants who received PMTCT should receive at least 6 months worth of guaranteed improved water and infant formula
What We Don’t Know: Research Needs • Safe water away from home. • Can sanitation alone or hygiene alone reduce diarrhea in PLWHAs? • Can improved WASH reduce the number of respiratory infections in PLWHAs? • Can improved WASH help maintain weight and nutritional status? • Can improved WASH provided at onset of symptoms delay the need for ART initiation? (delays resistance) • Can improved WASH prolong lifespan? • What has the water sector done internally to mitigate HIV/AIDS?
Job Site Programs • Involve employees and families • Management should take a lead role in • Mandatory sessions • Maintaining confidentiality • Offer services off-site if feasible • Programs should be evaluated and improved on a regular basis
Job Site Program Services • Education • BCC • Reducing stigma • Tackling sexual harassment in the workplace • Making people aware of company rules and benefits • Counseling and testing • Treatment • Care • Death benefits and survivor benefits