Download
1 / 52
520 likes | 551 Views
Learn about the normal absence of menstruation in women, including causes such as pregnancy, breastfeeding, and menopause. Explore menstrual disorders like dysmenorrhea, menorrhagia, amenorrhea, and oligomenorrhea, along with symptoms and treatments.

E N D
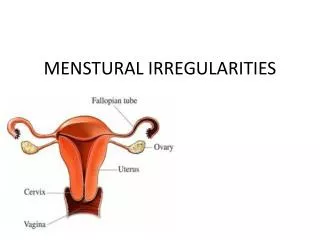
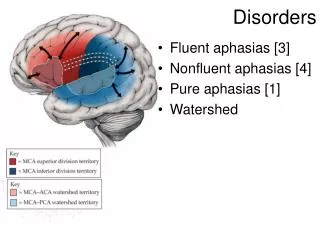
Reproductive Health NursingNUR 324 MENSTURAL DISORDERS Lecture 5
Normal Absence of Menstruation. Normal absence of periods can occur in any woman under the following circumstances: 1-Menstruation stops during the duration of pregnancy. Some women continue to have irregular bleeding during the first trimester. This bleeding may indicate a threatened miscarriage and requires immediate attention by the physician. 2- When women breastfeed they are unlikely to ovulate. After that time, menstruation usually resumes and they are fertile again. 3- Peri-menopause starts when the intervals between periods begin to lengthen, and it ends with menopause itself (the complete cessation of menstruation). Menopause usually occurs at about age 51, although smokers often go through menopause earlier.
Menstrual Disorders There are a number of different menstrual disorders. Problems can range from heavy, painful periods to no period at all.
Dysmenorrhea (Painful Cramps) • Painful menstrual cramps • Painful menses without evidence of a physical abnormality • Believed to be normal body response to uterine contractions
Dysmenorrhea (Painful Cramps) • Other symptoms : • Nausea, vomiting, gastrointestinal disturbances. • Prostaglandins cause forceful, frequent uterine contractions called cramps • Pain occurs in the lower abdomen but can spread to the lower back and thighs. • Dysmenorrhea is usually referred to as primary or secondary.
Primary dysmenorrhea • Cramps occur from contractions in the uterus. These contractions are a normal part of the menstrual process. • With primary dysmenorrhea, cramping pain is directly related to and caused by menstruation. • About half of menstruating women experience primary dysmenorrhea. • It usually begins two to three years after a women begins to menstruate. • pain typically develops when the bleeding starts and continues for up to 48 hours. • Cramps are generally most severe during heavy bleeding.
Secondary dysmenorrhea • Secondary dysmenorrhea is menstrually related pain that accompanies another medical or physical condition, such as endometriosis or uterine fibroids.
Dysmenorrhea: Treatment • Identify cause & manage pain • Analgesics & NSAIDS • Oral contraceptives • Diet changes: decrease salt, sugar, caffeine (fluid consumption); increase protein, Ca, Mg & Vit B • Balance rest & exercise
Menorrhagia (Heavy Bleeding) • During normal menstruation the average woman loses about (60 ml) or less of blood. Menorrhagia is the medical term for significantly heavier bleeding. • Menorrhagia occurs in 9 - 14% of all women and can be caused by a number of factors. • Women often overestimate the amount of blood lost during their periods.
Menorrhagia (Heavy Bleeding) • However, women should consult their doctor if any of the following occurs: 1- Soaking through at least one pad or tampon every hour for several hours. 2- Heavy periods that regularly last 10 or more days. 3- Bleeding between periods or during pregnancy.
Amenorrhea (Absence of Menstruation) • Amenorrhea is the absence of menstruation. There are two categories: primary amenorrhea and secondary amenorrhea. • These terms refer to the time when menstruation stops
Amenorrhea (Absence of Menstruation) Primary amenorrhea • occurs when a girl does not begin to menstruate. • Girls who show no signs of sexual development (breast development and pubic hair) by age 14 should be evaluated. • Girls who do not have their periods by two years after sexual development should also be checked. • Any girl who does not have her period by age 16 should be evaluated for primary amenorrhea.
Amenorrhea (Absence of Menstruation) Secondary amenorrhea • occurs when periods that were previously regular become absent for at least three cycles.
Oligomenorrhea(Light or Infrequent Menstruation) • Is a condition in which menstrual cycles are infrequent. It is very common in early puberty and does not usually indicate a medical problem. When girls first menstruate they often do not have regular cycles for a couple of years. • Even healthy cycles in adult women can vary by a few days from month to month. In some women, periods may occur every three weeks and in others, every five weeks.
Oligomenorrhea(Light or Infrequent Menstruation) • Flow also varies and can be heavy or light. • Skipping a period and then having • a heavy flow may occur; this is most likely due to missed ovulation rather than a miscarriage. Women should be concerned when periods come less than 21 days or more than three months apart, or if they last more than ten days. Such events may indicate ovulation problems.
Premenstrual Syndrome (PMS) Symptoms • Symptoms occur 7-10 days prior & are relieved when menstrual flow begins • inability to concentrate, depression, irritability, anxiety, mood swings, anger, aggressive behavior, acne, herpes recurrence, backache, edema, food cravings, wt. gain, increase susceptibility to infection. • Once established, the symptoms tend to remain fairly constant until menopause, although they can vary from cycle to cycle.
Premenstrual Syndrome (PMS) Pathophysiology • Not clearly understood; thought to be from hormonal fluctuations & increase in aldosterone • Aldosterone contributes to bloating & edema
Premenstrual Syndrome (PMS) Diagnosis • Must keep diary/calendar of symptoms for several months to make accurate diagnosis
Premenstrual Syndrome (PMS) Treatment • Management focuses on diet, exercise, relaxation & stress management • Diet high in complex CHO, Ca, Mg & Vit B • Diet low in sugar, caffeine & salt • Exercise & rest are both important • Relaxation techniques: breathing, meditation, relaxation.
Reproductive Health NursingNUR 324 UTERINE PROLAPSE Lecture 6
What is uterine prolapse ? Uterine prolapse is a condition in which a woman’s uterus (womb) slips out of its normal position . The uterus may slip enough that it drops part way into the vagina (birth canal) creating a lump or bulge . This is called incomplete prolapse -the uterus slips so far out of place that some of the tissue drops outside of the vagina . 21
GRADING UTERINE PROLAPSE GRADE 0: No prolapse GRADE 1: Descent towards vaginal introitus (>1cm above hymen) GRADE 2: Descent to vaginal introitus (hymen +/- 1cm from hymen) GRADE 3: Descent through introitus (> 1cm below hymen) GRADE 4: Prolapse totally outside introitus (uterine grade 4 = “procidentia”) 23
Bladder (Empty) 0 2 3 1 4 Rectum Hymen 1cm 1cm Figure 1: Prolapse staging – 0,1,2,3,4 (uterine – by the position of the leading edge of the cervix). Symphysis BH / JL 2007 Position: Section 2D (ii/iii) 24
Reproductive Pathophysiology GRADE 1 GRADE 2 26 GRADE 3 GRADE 4 W. Rose NURSING 621
The symptoms of uterine prolapse Women with mild cases of uterine prolapse may have no obvious symptoms. However ,as the uterus slip further out of position, it can place pressure on other pelvic organs--such as the bladder or bowel--causing a variety of symptoms, including: 27
Signs and Symptoms • Urinary frequency • Urinary urgency • Urinary incontinence • Nausea • Purulent discharge (rare) • Bleeding (rare) • Ulceration (rare) 28 Pelvic heaviness or pressure Pelvic pain Sexual dysfunction, including dyspareunia decreased libido Lower back pain Constipation Difficulty walking Difficulty urinating
Signs and Symptoms A protrusion of tissue from the opening of the vagina recurrent bladder infections Unusual or excessive discharge from the vagina Symptoms may be worsened by prolonged standing or walking. This is due to the added pressure placed on the pelvic muscles by gravity. 29
What causes uterine prolapse? The uterus is held in place within the pelvis by a group of muscles and ligaments. As these structures weaken, they become unable to hold the uterus in position, and it begins to sag. 30
What causes uterine prolapse? There are several factors that may contribute to the weakening of the pelvic muscles, including : Loss of muscle tone as the result of aging Injury during childbirth, especially if the woman has had many babies or large babies (more than 9 pounds) Other factors (obesity, chronic coughing or straining and chronic constipation all place added tension on the pelvic muscles, and may contribute to the development of uterine prolapse) 31
Pathophysiology Age Race (Hispanic) Pelvic structure (Anthropoid) Uterine structure Lifestyle (occupation) Multiparus Menopause Obstetrical trauma Decreased estrogen level Weakening of the pelvic tissues, muscles, ligaments 32
Uterine prolapse • Dysuria • Constipation • Urinary frequency • Nausea & vomiting • Urinary incontinence • Urinary urgency • Integumentary: • Protrusion of tissue • ulceration Stage I (descent to any point of the vagina above the hymenal remnants) • Reproductive: • Sexual dysfunction • Decreased libido • Musculoskeletal: • Pelvic heaviness • Pelvic pain • Low back pain Stage II (descent to the hymen) Stage III (descent beyond the hymen) • Circulatory: • Bleeding Stage IV (total eversion or procidentia) 33
Risk Factors of Uterine Prolapse? One or more pregnancies and vaginal births Giving birth to a large baby Increasing age Frequent heavy lifting Chronic coughing Frequent straining during bowel movements 34
How Common is Uterine Prolapse Uterine prolapse is fairly common and the risk of developing the condition increases with age. 35
Prevention Not to prolong the time of birth pay more than necessary. Non pressure on the uterus after childbirth. Sport after giving birth. Treat constipation. 36
Diagnoses The doctor will perform a pelvic examination to determine if the uterus has lowered from its normal position. During a pelvic exam, the doctor inserts a speculum (an instrument that lets the clinician see inside the vagina ) and examines the vagina and uterus. The doctor will feel for any bulges caused by the uterus protruding into the vaginal canal . 37
Treatment There are surgical and non-surgical options for treating uterine prolapse. The treatment chosen well as the woman’s general health, age and desire to have children. Treatment generally is effective for most women. Treatment options include the following: 38
Treatment A- Non surgical options 1.Exercise special exercise, called kegel exercise, can help strengthen the pelvic floor muscles. This may be the only treatment needed in mild cases of uterine prolapse. To do kegel exercise, tighten your pelvic muscles as if you are trying to hold back urine. Hold the muscle tight for a few seconds and then release. Repeat 10 times. You may do these exercise anywhere and any time (up to 4 times a day ) 39
Treatment A- Non surgical options 2-Vaginal pessary A pessary is a rubber or plastic doughnut-shaped device that fits around or under the lower part of the uterus and hold it in place. A health care provider will fit and insert the pessary , which must be cleaned frequently and removed before sex. 41
Treatment A- Non surgical options 3. Estrogen replacement therapy (ERT) Taking estrogen and other connective tissues that support the uterus. However, there are some drawbacks to taking estrogen, such as an increased risk of blood clots, gallbladder disease and breast cancer. The decision to use ERT must be made with your doctor after carefully weighing all of the risks and benefits. 43
Treatment B- Surgical options 1. Hysterectomy uterine prolapse may be treated by removing the uterus in a surgical procedure called hysterectomy. This may be done through an incision made in the vagina (vaginal hysterectomy) or through the abdomen (abdominal hysterectomy). Hysterectomy is major surgery , and removing the uterus means pregnancy is no longer possible. 44
Treatment B- Surgical options 2. Uterine suspenstion This procedure involves putting the uterus back into its normal position. This may be done by reattaching the pelvic ligaments to the lower part of the uterus to hold it in place. Another technique uses a special material that acts like a sling to support the uterus in its proper position. Recent advances include performing this with minimally invasive techniques and laparoscopically (through small band aid sized incisions) that decrease post operative pain and speed recovery . 45
Complications If left untreated, uterine prolapse can interfere with bowel, bladder and sexual functions. Infection Prolapse of other pelvic organs-including rectum and bladder A prolapsed bladder bulges into the front part of vagina, causing a cystocele that can lead to difficulty in urinating and increased risk of urinary tract infection . A prolapsed rectum causes a rectocele, which often leads to uncomfortable constipation and possibly hemorrhoids . 46
Prevention Of Uterine Prolapsed It may not be possible to prevent all cases of uterine prolapse, but there are steps that can be taken to help reduce the risk: Maintain a healthy body weight Exercise regularly (for 20 to 30 minutes, three to five times per week), including kegel exercise, which may done up to four times a day . Be sure to check with your health care provider before starting any new exercise program . 47
Nursing management 48 preventive measures: 1. Early visits to HC provider = early detection 2. Teach Kegel’s exercises during postpartum period preoperative nursing care: 1. Thorough explanation of procedure, expectation and effect on future sexual function 2. Laxative at home a day prior procedure 3. Perineal shave prescribed also 4. Lithotomy position for surgery
Nursing management 49 postoperative nursing care: Pt. is to void few hours after surgery; catheter if unable (after 6 hrs) Pain 1. Administer analgesic as prescribed. 2. Provide comfort measures such as backrub.
Constipation 50 1. Administer stool softeners/laxatives as prescribed. 2. Encourage increase in fluid and fiber intake. 3. Encourage early ambulation.