Download
1 / 33
400 likes | 783 Views
Brachial Plexus Birth Palsy. Alireza Pahlevansabagh M.D. T.U.M.S . Etiology Risk factors Anatomy Clinical Features Classification Prognosis and Natural History Differential Diagnosis. Etiology.

E N D
Brachial Plexus Birth Palsy Alireza Pahlevansabagh M.D. T.U.M.S.
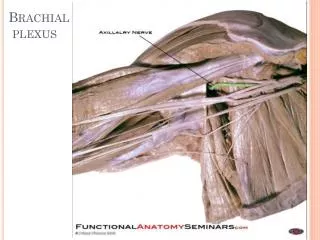
Etiology • Risk factors • Anatomy • Clinical Features • Classification • Prognosis and Natural History • Differential Diagnosis
Whereas a mechanical basis for BPBP is well accepted, delivery by cesarean does not exclude the possibility of birth palsy.
EPIDEMIOLOGY • Brachial plexus birth palsy has an incidence of 0.4 to 4per 1000 live births. • Most common on the right side
RISK FACTORS • large size for gestational age (macrosomia) • shoulder dystocia • maternal short stature • maternal diabetes • breech delivery • multiparous pregnancies • previous deliveries resulting in BPBP • prolonged labor • assisted (vacuum or forceps) deliveries
Clinical Features • Lack of movement of the affected arm usually leads to referral for orthopaedic opinion.
ClassificationNarakas et al. • Group I classic uppertrunk lesion C5-6 • Group II extended upper trunk lesion C5-7 • Group III flail extremity • Group IV flail extremity +Horner’s syndrome
Group I absence of shoulder abduction and external rotation, elbow flexion, and forearm supination. • spontaneous recovery 90%
Group II with the absence of wrist and digital extension added to the limitations noted in group I
Group III consists of a flail extremity but without Horner's syndrome.
Group IV is manifested as a flail extremity and Horner’s syndrome. These infants may have an associated phrenic nerve palsy
Prognosis and Natural History • it is important to determine whether the injury is preganglionic or postganglionic.
Horner's syndrome (sympathetic chain) • elevated hemidiaphragm (phrenic nerve) • winged scapula (long thoracic nerve) • absence of rhomboid (dorsal scapular nerve) • lower plexus involvement • upper trunk lesion seen with a breech delivery • complete palsy • lower Iimb weakness or spasticity
Infants who recover partial antigravity upper-trunk muscle strength in the first 2 months of life should have a full and complete neurologic recovery over the first 1 to 2 years of life
Cases in which the return of biceps function occurs after 3 months rarely have complete recovery without some notable limitations in strength or range of motion.
Muscle imbalance develops rapidly, and soft tissue contracture contributes to deformity and joint incongruence early in the neonatal period.
lengths of the affected limbs were compared with the unaffected side • upper arm 95%, • forearm 94% • hand 97%
These children participate in sports at the same rate as their peers. • There was no increased injury rate for these children
Differential Diagnosis • fracture of the clavicle or humerus • proximal humeral physeal separation • septic arthritis of the shoulder • acute osteomyelitis • congenital malformation of the plexus • tumors involving the spinal cord or plexus