Download
1 / 44
480 likes | 1.19k Views
Brachial Plexus. Dr. Sama-ul-Haque Dr. Nivin Sharaf. BRACHILAL PLEXUS.

E N D
Brachial Plexus Dr. Sama-ul-Haque Dr. Nivin Sharaf
BRACHILAL PLEXUS • The brachial plexus is a somatic nerve plexus formed by intercommunications among the ventral rami of the lower four cervical nerves ( C 5 - C 8) and the first thoracic nerve (T 1). The plexus is responsible for the motor innervation to all of the muscles of the upper limb with the exception of the trapezius and levator scapula.), and the sensory innervation of the upper limb except an area just above the point of the shoulder (supplied by supraclavicular nerves) and the dorsal scapular area which is supplied by cutaneous branches of dorsal rami.
FORMATION OF THE BRACHIAL PLEXUS • Roots • The ventral rami of spinal nerves C5 to T1 are referred to as the roots of the plexus. • Trunks • Shortly after emerging from the intervertebral foramina , these 5 roots unite to form three trunks. • The ventral rami of C5 & C6 unite to form the Upper Trunk. • The ventral ramus of C 7 continues as the Middle Trunk. • The ventral rami of C 8 & T 1 unite to form the Lower Trunk. • Divisions • Each trunk splits into an anterior division and a posterior division. • The anterior divisions usually supply flexor muscles • The posterior divisions usually supply extensor muscles
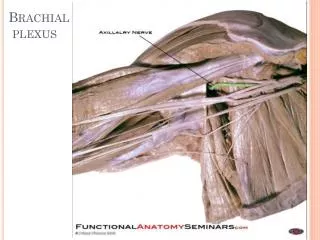
FORMATION OF THE BRACHIAL PLEXUS CONT. • Cords • The anterior divisions of the upper and middle trunks unite to form the lateral cord. • The anterior division of the lower trunk forms the medial cord. • All 3 posterior divisions from each of the 3 cords all unite to form the posterior cord. • The cords are named according to their position relative to the axillary artery • Terminal branches: • Musculo Cutaneous • Ulnar n. • Median n. • Axillary n. • Radial n.
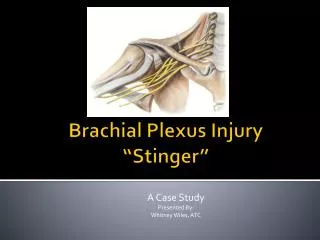
Brachial Plexus Injuries • The brachial plexus lies in the posterior triangle of the neck between the scalenus anterior and scalenus medius muscles. At the root of the neck, it lies behind the clavicle. • The most common injury is severe traction with the arm in abduction e.g. after a motor cycle accident. Partial paralysis may also result from shoulder dislocation. Direct injury to the brachial plexus can result from a stab or gunshot wound. :
Brachial Plexus Injuries • In Adults: • Sports most commonly associated: Football, baseball, basketball, volleyball, wrestling, and gymnastics. • Nerve injuries can result from: Blunt force trauma, poor posture or chronic repetitive stress.
Brachial Plexus Injuries • Patients generally present with pain and/or muscle weakness. • Some patients may experience muscle atrophy.
Brachial Plexus Injuries Result: Anesthesia Paralysis 1. Complete 2. Incomplete
Erb- Duchenne palsy Injury to Superior part of Plexus. Occurrence: Due to excessive increase in the angle between neck and the shoulder. Roots Involved: C5 and C6 Muscles Involved: Shoulder Arm
What is Waiter’s tip or Porter’s tipposition?
Erb- Duchenne palsy Clinical Appearance: Motor Loss: Adducted Shoulder Medially Rotated Arm Extended Elbow Sensory Loss: Lateral aspect of Upper Limb (uncommon)
Waiter’s tip position • Characteristic position - adduction and internal rotation of the arm with forearm pronated • Forearm extension normal • Biceps reflex absent
Waiter’s tip palsy • Erb's palsy is caused by damage to the brachial plexus during delivery of the neonate. This is mostly limited to the 5th and 6th cervical nerves
klumpke paralysis or Palsy Injury to Inferior part of Plexus. Occurrence: Excessive abduction of arm. Less common then Injury to Superior part of Plexus. Roots Involved: C8 and T1
klumpke paralysis or Palsy Clinical Appearance: Motor Loss: Small muscles of Hand Sensory Loss: Medial aspect of Upper Limb
Claw Hand Aetiology: brachial plexus lesion (C8-T1),Ulnar, and/ or Median nerve injury This occurs when all fingers are clawed. It is the result of hyperextension at the metacarpophalangeal joints and flexion of the interphalangeal joints.
Cervical Rib Involves Inferior part of Plexus
References • http://www.upstate.edu/cdb/education/grossanat/limbs2.shtml • www.medicalstudent.com • www.netteranatomy.com