Download
1 / 40
550 likes | 958 Views
Bone Density : A Key Determinant for Treatment Planning. Presented by:Dr.Mahsa Sahraneshin Supervised by: Dr. Mansour Rismanchian And Dr.saied Nosouhian Dental of implantology Dental implants research center Isfahan university of mediacal science.

E N D
Bone Density: A Key Determinant forTreatment Planning Presented by:Dr.MahsaSahraneshin Supervised by: Dr. MansourRismanchian And Dr.saiedNosouhian Dental of implantology Dental implants research center Isfahan university of mediacal science
Bone Density: A Key Determinant forTreatment Planning Chapter 7 By MahsaSahraneshin
Available bone is particularly important in implant and describes: the external architecture orvolume of the edentulous area considered for implants. • Today, the treatment plan first considers the final prosthesis options. The patient force factors are then noted. • The density of available bone in an edentulous site is a determining factor in • treatment planning, • implant design, • surgical approach, • healing time, • and initial bone loading during prosthetic reconstructlon.
INFLUENCE OF BONE DENSITY ON IMPLANT SUCCESS RATES • The reduced implant survival : • Poor bone quality, especially when coupled with poor bone volume (65% of these patients experienced failure). • often is related to bone density than arch location(more failure in maxilla &Posterior zone). • are not primarily related to surgery healing, but instead occur after prosthetic loading.
ETIOLOGY OF VARIABLE BONE DENSITY • Bone change in relation to a number of factors : • hormones • vitamins • mechanical influences • biomechanical parameters, such as duration of edentulous state, are predominant. Wolff, in 1892, published, "Every change in the form and function of bone or of its function alone is followed by certain definite changes in the internal architecture. "
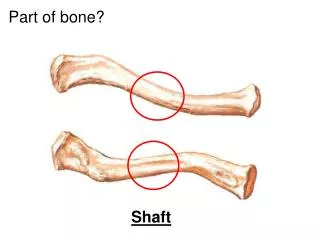
the bone is most dense around the teeth(cribriform plate) and more dense around the teeth at the crest, compared with the apices . • Generalized trabecular bone loss occurs in regions around a tooth from a decrease in mechanical strain. a decrease in the trabecular bone pattern around a maxillary molar with no opposing occlusion(left), compared with a tooth with occlusal contacts on the contralateral side .
Bone density in the jaws decreases after tooth loss. This loss is related to : The length of time the region has been edentulous and not loaded . the initial density of the bone flexure and torsion in the mandible and parafunctionbefore and after tooth loss. the density change after tooth loss is greatest in the posterior maxilla and least in the anterior mandible.
bones are constantly modified by modeling or remodeling . • Modelinghasindependent sites of formation and resorption and results in the change of the shape or size of bone. • Remodelingis a process of resorption and formation at the same site that replaces previously existing bone and primarily affects the internal turnover of bone,. • region where teeth are lost . • bone next to an endosteal implant. • The greater stress applied to the bone the greater strain in the bone. • Bone modeling and remodeling are primarily controlled, by the mechanical environment of strain. • The density of alveolar bone is a result of mechanical deformation from microstrain. Frost proposed a model of 4 histologic patterns for bone as it relates to mechanical adaptation to strain. The pathologic overload zone mild overload zone adapted window acute disuse window
lowest microstrain amount causes increase in fatigue fractures, remodeling, and bone resorption . ideal physiologic loading zone causes microfracture and triggers an increase in bone remodeling, which produces more woven bone .
acute disuse window • The bone loses mineral density . • modeling for new bone is inhibited and remodeling is stimulated with a gradual net loss of bone. • The microstrain of bone for trivial loading is reported to be 0 to 50 . • This phenomenon may occur throughout the skeletal system, as evidenced by a 15% decrease in the cortical plateand extensive trabecular bone loss consequent to immobilized limbs for 3 months. • cortical bone density decrease of 40% . and • trabecular bone density decrease of 12% .
adapted window • The adapted window (50 to 1500 microstrain) represents an equilibrium of modeling and remodeling, and bone conditions are maintained at this level. • Bone in this strain environment remains in a steady state, and this may be considered the homeostatic window of health. • The histologic description of this bone is primarily lamellar or load-bearing bone. • Approximately 18% of trabecular bone and 2% to 5% of cortical bone is remodeled eachyear in the physiologic loading zone, which corresponds to the adapted window. • This is the range of strain ideally desired around an endosteal implant .
Pathologic overload zones mild overload zone • Pathologic overload zones are reached when microstrains are greater than 3000 units. • Cortical bone fractures occur at 10,000 to 20,000 microstrain(1% to 2% deformation). so pathologic overload may begin at microstrain levels of only 20% to 40% of the ultimate strength . • The bone may resorb and form fibrous tissue, or repair woven bone. • The marginal bone loss evidenced during implant overloading may be a result of the bone in the pathologic overload zone . The mild overload zone (1500 to 3000 microstrain) causes a greater rate of fatigue microfraeture and increase in the cellular turnover rate of bone. The bone strength and density may decrease. The histologic description of bone is woven or repair bone. The state for bone when an endostealimplant is overloaded. During the repair process, the woven bone is weaker than the more mature, mineralized lamellar bone. so while bone is loaded in the mild overload zone, care must be taken because bone strength is reduced during the repair.
BONE CLASSIFICATION RELATED TO IMPLANT DENTISTRY • classified bone density into 3 categories: • Class I : This ideal bone type consists of evenly spaced trabeculae with small cancellated spaces. • Class II : The bone has slightly larger cancellated spaces with less uniformity of the osseous pattern. • Class III : Large marrow-filled spaces exist between bone trabeculae. • Class III bone results in a loose-fitting implant; • Class II bone was satisfactory for implants; • Class I bone was the most ideal foundation for implant prostheses. Quality 1 →homogeneous compact bone. Quality 2 → had a thick layer of compact bone surrounding a core of dense trabecular bone. Quality 3 → had a thin layer of cortical bone surrounding dense trabecular bone of favorable strength. Quality 4 → had a thin layer of cortical bone surrounding a core of low density trabecular bone.
MISCH BONE DENSITY CLASSIFICATION • D1 is dense cortical bone. • D2 has dense-to-porous cortical bone on the crest and, within the bone, has coarse trabecular bone. • D3 have a thinner porous cortical crest and fine trabecular bone. • D4 has no crestal cortical bone. The fine trabecular bone composes all of the total volume of bone. • D5 A very soft bone, with incomplete mineralization and large interterabecular spaces. is most often immature bone in a developing sinus graft.
The bone density may be determined by tactile sense during surgery the general location radiographic evaluation.
D1 bone : • never observed in the maxilla and is rarely observed in mandibles. • in the anterior mandible • in the anterior and posterior mandible, when the implant is engaging the lingual cortical plate of bone. • C-h bone volume (moderate atrophy) in the anterior . • D2 Bone : • the most common bone density in the mandible . • The anterior mandible consists of D2 bone 2/3 of the time. • Almost half of patients have D2 bone in the posterior mandible. • The maxilla presents D2 bone less often than the mandible. • ¼ of patients have D2 bone, and this is more in the : • partially edentulous patient's anterior and premolar region. • Single-tooth or 2-tooth, partially edentulous spans in either arch almost always have D2 bone.
The softest bone, D4: • most often in the posterior maxilla ,especially in the molar regions or after a sinus graft augmentation . • The anterior maxilla has D4 bone less than 10% of the time-more often after an onlay iliac crest bone graft. • When observed in mandible, it is usually in a long-term, completely edentulous patient after an osteoplasty to remove the crestal bone. D3: • very common in the maxilla. • More than half the patients have D3 bone in the upper arch. • The anterior edentulous maxilla has D3 bone about 75% of the time, whereas almost half the patients have posterior maxillae with D3 bone (more often in the premolar region). • Almost half of the posterior mandibles present with D3 bone, whereas approximately 25% of the anterior edentulous mandibles have D3 bone.
It is safer to err on the side of less dense bone during treatment planning, so the prosthesis will be designed with slightly more, rather than less, support. • the initial treatment plan before computed tomographic(CT) radiographic scans or surgery suggests : • anterior maxilla is treated as D3 bone, • the posterior maxilla as D4 bone, • the anterior mandible as D2 bone, • and the posterior mandible as D3 bone.
RADIOGRAPHIC BONE DENSITY • the initial treatment plan, often begins with Periapical or panoramic radiographs.but • the lateral cortical plates often obscure the trabecular bone density. • the more subtle changes of D2 to D3 cannot be quantified by these. • CT produces axial images of the patient's anatomy, perpendicular to the long axis of the body. Each CT axial image has 260,000 pixels, and each pixel has a CT number (Hounsfield unit) related to the density of the tissues . • the higher the CT number, the denser the tissue. • Modern CT scanners can resolve objects less than 0.5 mm apart. • The very soft bone observed after some bone grafts may be 50 to 200 units. Negative numbers fat tissue. In the mandible, failed sites exhibited higher Hounsfield numbers. due to the lack of vascularization or overheating during surgery. By contrast, in the maxilla, the bone density was low for the failed sites. The bone density may be different from the crest, to the apical . The most critical region of bone density is the crestal 7 to 10 mm of bone. when the bone density , the crestal 7 to 10 mm determines the treatment plan protocol.
BONE DENSITY-TACTILE SENSE • Site preparation and implant placement in • D1 : drill preparing an osteotomy in oak or maple wood. • D2 bone is similar to the tactilesensation of drilling into white pine or spruce. • D3 bone is similar to drilling into a compressed balsa wood. • D4 bone is similar to drilling into compressed Styrofoam or a light balsa wood. • In D4 bone, the drill may be inserted to the full desired depth without the drill rotating. a bone compression rather than extraction process may be used with the drill. • D3 bone is very easy to prepare, but requires the drill to rotate while it is pressed into position.
SCIENTIFIC RATIONALE OF A BONE DENSITY-BASED TREATMENT PLAN • Bone Strength and Density • Elastic Modulus and Density • Bone Density and Bone-Implant Contact Percentage • Bone Density and Stress Transfer
Bone Strength and Density • D2 bone exhibited a 47%to 68% greater ultimate compressive strength, compared with D3 bone. • on a strength scale of 1 to 10: • D1 bone is a 9 to 10 relative to strength. • D2 bone is a 7 to 8 on this scale. • D3 bone is 50% weaker than D2 bone and is a 3 or 4 on the strength scale. • D4 bone is a 1 to 2 (up to 10 times weaker than D1 bone .)
Clinical failure was predicted in D4 bone and some D3 densities under occlusal loads.
Elastic Modulus and Density • bone is more flexible than titanium. • The difference between the two materials may create microstrain conditions of pathologic overload and cause implant failure .
When higher stresses are applied to an implant prosthesis, the titanium has lower strain (change in shape) compared with the bone. When the stresses applied to the implant are low, the microstrain difference between titanium and bone is minimized and remains in the adapted window zone, maintaining load bearing lamellar bone at the interface
the elastic modulus in the human jaw to be different for each bone density. • when a stress is applied to an implant in D1 bone, the titanium-D1 bone interface exhibits very small microstraindifference. • In comparison, when the same amount of stress is applied to an implant in D4 bone, the microstrain difference between titanium and D4 bone is greater and may be in the pathologic overload zone .
Bone Density & Bone-Implant Contact Percentage • The bone implant contact (BIC) percentage is greater in cortical bone . • The very dense D1 bone of a C-h resorbed anterior mandible or of the lingual cortical plate of a Division A anterior or posterior mandible →the highest percentage of bone in contact with implant ( more than 85% BIC.) • D2 bone, after initial healing→65% to 75% BIC. • D3 bone →40% to 50% BIC after initial healing . • The sparse trabeculae of the bone often found in the posterior maxilla (D4) offer fewer areas of contact with the body of the implant. greater implant surface area is required to obtain a similar amount of bone-implant contact in soft bone, compared with a denser bone quality found around an anterior mandibular implant.
BIC D2 D1 D4 D3
Bone Density and Stress Transfer • Crestal bone loss & early implant failure after loading may occur from excess stress at the implant-bone interface. • In D1 bone, highest strains are concentrated around the implant near the crest. • D2 bone, with the same load, sustains a slightly greater crestal strain, and the intensity of the stress extends farther apically along the implant body . • D4 bone exhibits the greatest crestal strains , and the magnitude of the stress on the implant proceeds farthest apically along the implant body.
following 3 different clinical situations at the bone-implant interface, may occure , based on bone density: (1) physiologic bone loads in the adapted window zone and no marginal bone loss (2) mild overload to pathologic overload bone loads and crestal bone loss, or (3) generalized pathologic overload and implant failure.
4 facts form the basis for treatment plan modification in function of the bone quality: (1) each bone density has a different strength; (2) bone density affects the elastic modulus; (3) bone density differences result in different amounts of bone-implant contact percent; (4) bone density differences result with a different stress-strain distribution at the implant-bone interface.
One way to reduce the biomechanical loads on implants is by prosthesis design to decrease force. For example : • cantilever length may be shortened or eliminated, • narrower occlusal tables designed . • offset loads minimized . • RP-4 restorations, permit the patient to remove the restorations at night and reduce parafunctional forces. • RP-5 prostheses permit the soft tissue to share the occlusal force and reduce the stress on the implants. • As the bone density decreases, these prosthetic factors become more important.
Stress reduced by : In D2 bone with normal patient forces, a pontic may replace a tooth between two implants. In D3 bone, one implant per tooth is often appropriate • A load directed along the long axis of the implant body. • A load directed along the long axis of the implant body decreases the amount of stress in the crestal bone . 2 ) increasing the functional area over which the force is applied: • Increasing implant number is an excellent way to reduce stress by increasing functional loading area. • 3 implants rather than 2 may decrease applied implant moments in ½ and bone reaction forces by 2/3. • An implant prosthesis with normal patient forces in the bone should have at least one implant per tooth. • In the molar region , 2 implants for each missing molar is appropriate.
3 ) Increase Width and length of the implant : • For every 0.5 mm increase in width, there is an increased surface area between 10% and 15% for a cylinder implant, and even more difference is found with threaded-implant body designs . • Because the greatest stresses are concentrated at the crestal region of the implant, width is more significant than length . • D4 bone should often require wider implants : This may require onlay grafts or bone expansion to increase the width of bone. • the minimum bone height for initial fixation and early loading (using the classic V-threadscrew implant design and titanium surface condition ) : • D1 bone , 7mm • D2 bone, 9 mm • D3 bone, 12 mm
4 ) macro design of implant : Implants designed for D4 bone should have the greatest surface area. For example, a classic V-thread screw design has 30% more surface area than a cylinder implant. 5 ) The depth of the thread : • The deeper the thread depth in the implant body, the more functional surface area for the bone implant contact. An implant body designed for the soft bone should have more and deeper threads . 6 ) Coatings or the surface condition on an implant A rougher surface is strongly suggested in soft bone and has resulted in improved short-term survival rates. After 1 to 2 years, the mechanical load on the overall implant design is more critical to the amount and type of bone contact compared with the surface condition on the implant body.
Rough surface conditions Disadvantages: • Plaque retention when exposed above the bone • contamination • and increased cost. • The benefit and risk of surface conditions suggests the roughest surfaces are most often used in only softer bone types. 7 ) Progressive bone loading • allow the bone to mature and accommodate to the local strain environrment. • Over time, progressive loading changes the amount and density of the implant bone contact improves support. • The softer the bone, the more important the need for progressive loading.