Download
1 / 116
1.43k likes | 2.64k Views
Principles of Fracture Treatment. What is a (bony) fracture?. Disruption of a bone’s normal structure or “wholeness” Crack, break, or rupture in a bone There are many how’s and why’s to bony fractures Terms used to describe each are related. Definition of Fracture.

E N D
What is a (bony) fracture? • Disruption of a bone’s normal structure or “wholeness” • Crack, break, or rupture in a bone • There are many how’s and why’s to bony fractures • Terms used to describe each are related
Definition of Fracture • There are 2 types of # in which this is not so: • Pathological fract. • Stress fract.
Pathological fracture : It is one in which a bone is broken through an area weakened by pre-existing disease , & by a degree of force that would have left normal bone intact e.g osteoporosis , O.M. , bone tumours.
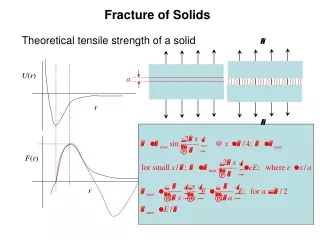
Stress fracture : Bone, like other materials, reacts to repeated loading. On occasion, it becomes fatigued & a crack develops e.g military installations, ballet dancers & athletes.
Diagnosis • Clinical picture • Radiography
Clinical Features of Fracture • History of trauma • Symptoms & signs: 1. Pain & tenderness 2. Swelling 3. Deformity 4. Crepitus 5. Loss of function 6. Abnormal move. 7. N.V. injuries
Orthopaedic History • A good general orthopaedic history contains: • Onset, Duration, and Location of a problem • Limitations and debilitation attributed to the problem • Good surgical history, especially with regards to orthopaedic surgeries and prior anesthesia • Co-morbid conditions that contribute to the problem or will preclude healing in some manner
Physical Exam Basics • Inspect and Palpate everything- start with normal structures and move to abnormal • Range of motion in all planes • Strength • Sensation • Reflexes • Gait • Stability
Physical Exam Basics • NVI What does this mean? • Neurologic exam- Always document the neurologic status. Some fractures are associated with nerve injuries and knowing the status of the nerve is critical • Vascular exam- Always check for pulses distal to the fracture sight. Missed vascular injuries can be devastating
Pre-reading Musculoskeletal Radiographs • 1: Name, date, old films for comparison • 2: What type of view(s) • 3: Identify bone(s) & joint(s) demonstrated • 4: Skeletal maturity (physes: growth plates) • 5: Soft tissue swelling • 6: Bones & joints (fractures & dislocations)
Physical Exam • NEVER trust someone else’s exam. ALWAYS put your hands on the patient and see for yourself • Always trust your exam- you WILL pick up something that someone else has missed at some point
Intro to Reading X-rays • Reading a radiograph is essentially describing the anatomy of a certain structure • In order for it to be universal and understandable for others, clarity and precision are essential • A fracture is described based on the findings of the physical exam and a review of radiographs
Reading X-rays • Say what it is- what anatomic structure are you looking at and how many different views are there • Regional Location- Diaphysis (rule of 1/3), Metaphysis, Epiphysis including intra and extra-articular • Direction of the fracture line- Transverse, Oblique, Spiral
Reading X-rays • Condition of the bone- comminution (3 or more parts), Segmental (middle fragment), Butterfly segment, incomplete, avulsion, stress, impacted • Deformity-Displacemtent (distal with respect to proximal), angulation (varus, valgus), rotation, shortening (in cm’s), distraction
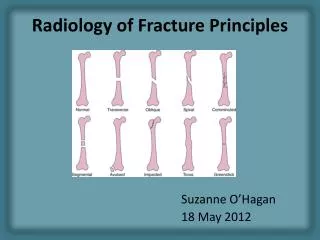
Fracture Pattern • Transverse • Produced by a distracting or tensile force
Fracture Pattern • Spiral • Produced by a torsional force
Fracture Pattern • Produced by pure bending force • Butterfly
Fracture Pattern • Comminuted • Broken into many pieces- high energy with combined forces
Displacement • Characterized by % of bone contact on either view
Angulation • Distal fragment relative to proximal • Varus, Valgus, Anterior, Posterior • Apex of angle formed by fragments • E.g., Apex Anterior, Apex Medial, Apex Ulnar
Location • Commonly described in thirds of affected bone • ie distal third of tibia • ie junction of proximal and middle third of femur • If fractured at two levels describe as segmental
Location-Diaphysis • Shaft portion of bone
Location-Metaphysis • The ends of the bone (if the fracture goes into a joint it is described as intra- articular)
Now All Together • Transverse fracture of the femur at the middle third- distal third junction with 100% displacement and varus (or apex lateral) angulation
Mnemonic: OLD ACID • O: Open vs. closed • L: Location • D: Degree (complete vs. incomplete) • A: Articular extension • C: Comminution / Pattern • I: Intrinsic bone quality • D: Displacement, angulation, rotation
O: Open vs. Closed • Open fracture • AKA: “Compound fracture” • A fracture in which bone penetrates through skin; • “Open to air” • Some define this as a fracture with any open wound or soft tissue laceration near the bony fracture • Closed fracture • Fracture with intact overlying skin
L: Location Epiphysis • Which bone? • Thirds (long bones) • Proximal, middle, distal third • Anatomic orientation • E.g. proximal, distal, medial, lateral, anterior, posterior • Anatomic landmarks • E.g. head, neck, body / shaft, base, condyle • Segment (long bones) • Epiphysis, physis, metaphysis, diaphysis Physis Metaphysis Diaphysis (Shaft) Articular Surface
D: Degree of Fracture • Complete • Complete cortical circumference involved • Fragments are completely separated • Incomplete • Not fractured all the way through • “Only one cortex” involved • e.g “Greenstick fracture”
A: Articular Extension / Involvement • Intra-articular fractures • “Involves the articular surface” • Dislocation • Loss of joint surface / articular congruity • Fracture-dislocation
C: Comminution / Pattern • Transverse (Simple) • Oblique (Simple) • Spiral (Simple) • Linear / longitudinal • Segmental • Comminuted • Compression / impacted • “Buckle / Torus” • Distraction / avulsion
C: Comminution / Pattern • Transverse (Simple)
C: Comminution / Pattern • Oblique (Simple) • Spiral (Simple) • Oblique in 2+ views
C: Comminution / Pattern • Linear / longitudinal / split
C: Comminution / Pattern • Segmental • Bone broken in 2+ separate places; Fx lines do not connect
C: Comminution / Pattern • Comminuted • Broken, splintered, or crushed into >3 pieces
C: Comminution / Pattern • Compression • Impacted • (e.g. “Buckle / Torus”)
C: Comminution / Pattern • “Buckle / Torus”
C: Comminution / Pattern • Distracted • Avulsion
I: Intrinsic Bone Quality Normal • Osteopenia • Decr’d density
I: Intrinsic Bone Quality • Osteopetrosis • Incr’d density Normal
I: Intrinsic Bone Quality Normal • Osteopoikilosis • Focal areas of incr’d density
D: Displacement, Angulation, Rotation • Displacement • Extent to which Fx fragments are not axially aligned • Fragments shifted in various directions relative to each other • Convention: describe displacement of distal fragment relative to proximal Oblique tibial shaft Fx b/w distal & middle thirds; laterally displaced
D: Displacement, Angulation, Rotation • Angulation • Extent to which Fx fragments are not anatomically aligned • In a angular fashion • Convention: describe angulation as the direction the apex is pointing relative to anatomical long axis of the bone (e.g. apex medial, apex valgus) R Tibial shaft Fx b/w prox & middle thirds, angulated apex lateral (apex varus)