Download
1 / 60
600 likes | 860 Views
TMJ Disorders and its management. Prof.Dr . Ahlam El- Sharkawy Head of prosthodontic departement Pharos University in Alexandria. What is the Temporomandibular Joint?. Temporomandibular joint represents the articulation of the mandible to the temporal bone of the cranium.

E N D
TMJ Disorders and its management Prof.Dr. Ahlam El-Sharkawy Head of prosthodonticdepartement Pharos University in Alexandria
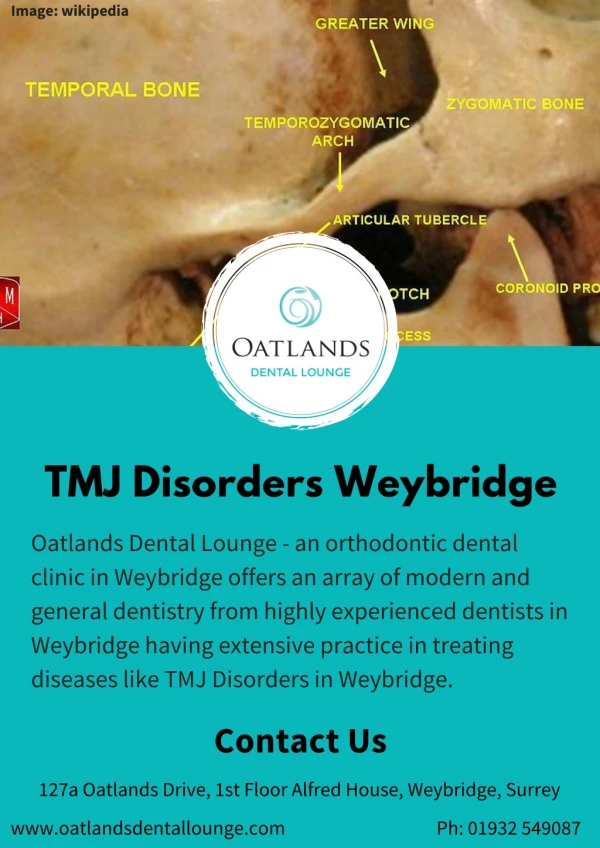
What is the Temporomandibular Joint? • Temporomandibular joint represents the articulation of the mandible to the temporal bone of the cranium.
What is the Temporomandibular Joint? • Interarticular disc lies between the mandibular condyle and the temporal bone, helping in smooth motion. • This disc absorbs shocks to the jaw joint from chewing and other movements.
TMJ innervation : - Sensory supply through the auriculotemporal nerve branch from the mandibular nerve branch from the trigeminal nerve. - Motor supply to the muscles through the mandibular nerve (the main trunk and the anterior division).
Normal closed and opened positions jaw opened jaw closed
TMJ Disorders Temporomandibular disorder (TMD) is a collective term used for a number of clinical problems that involve the masticators muscle, TMJ, and/or associated structures. The term TMD has been defined as an abnormal, incomplete or impaired function of the TMJs.
Classification TMD fall into two main categories: Myogenous , which involves muscles. Arthrogenous , which involves articular bones, or disc inbetween.
Articulardisorders “arthrogenous Degenerative disk disorders Inflammatory; capsulitis, synovitis, polyarthiritides. Non-inflammatory; osteoarthritis
Articulardisorders “arthrogenous” Disk derangement disorders Displacement with reduction. Displacement without reduction [closed lock]. Perforation. Dislocation(open-lock)
Common sign and symptoms • the most common initial symptom is 1- pain, usually localized in • Muscles of mastication • The preauricular area • TMJ • May radiate to head and neck • And aggravated by chewing or other jaw functions.
Common sign and symptoms • 2-Limited mandibular movements, • 3-joint noises( clicking, creptius ) • 4-jaw ache, ear ache, headache, and facial pain.
Etiological factors 1- Tensional, emotional ,and physical stress. 2-Occlusal interference, premature contact and occlusal instability. 3-Pain in masticatory system. 4-Abnormal biting habits. 5-loss of posterior teeth. 6-External force or trauma. 7-Pathophysiologic factors.
Examination of TMD 1. History 2.Clinical examination 3. Radiographic examination
Examination of TMD1.history Personal history: including patient's name, age, sex, occupation, marital status, telephone number and habits such as bruxism. Medical history: to exclude systemic diseases affecting bone, joint and /or muscles.
Examination of TMD1.history Dental history: To detect any relation between dental procedures and the onset of the TMJ symptoms, also if there is any history of trauma to jaw .
Examination of TMD1.history • Chief complaint: • The most imp in history the type of pain(usually dull pain) location, onset, characteristics, aggravating factors • So treatment must be directed toward the source of pain, not to the site where it is felt.
Examination of TMD II-Clinical examination: The masticatory apparatus examination consists of evaluating three major structures: muscles joints teeth.
II.Clinical examination of TMD1. Muscles examination 1.Temporalis The temporalis muscle is segmented into anterior, middle, and posterior regions. 1.Temporalis (anterior): Fibers of this region run vertically and were palpated above the zygomatic arch and anterior to the TMJ.
II.Clinical examination of TMD1. Muscles examination Temporalis (middle): Fibers of theses region run obliquely and were palpated in the depression above the TMJ about 2cm lateral to the lateral border of the eyebrow
II.Clinical examination of TMD1. Muscles examination Temporalis (posterior): Fibers of this region run horizontally and were palpated above and behind the ear.
II.Clinical examination of TMD1. Muscles examination Masseter: The masseter is palpated by placing the fingers on the zygomatic arch then they are dropped down slightly just anterior to the joint.
II.Clinical examination of TMD1. Muscles examination Lateral ptrygoid muscle: palpated by placing the index finger on the lateral side of the alveolar ridge above the maxillary molars while moving the finger upward and medial to palpate. (the location for the posterior superior alveolar injection)
II.Clinical examination of TMD1. Muscles examination Medial pterygoid muscle: Slide the index finger a little posterior to the traditional insertion site for an inferior alveolar injection, until you feel muscle, and press laterally. to where muscle is felt and press laterally.
II.Clinical examination of TMD1. Muscles examination Sternomastoid: Bilaterally palpate the sternomastoid muscles by squeezing each between the thumb and index finger along the length of the muscle.
II.Clinical examination of TMD3. joint examination Palpation of TMJ Range of motion TMJ noise
II.Clinical examination of TMD3. joint examination Palpation of TMJ TMJ needs to be palpated in two locations. Tenderness in one of these locations is not necessarily associated with tenderness in another. Palpate the first location by asking the patient to open approximately 20 mm and palpating the condyle’s lateral pole.
II.Clinical examination of TMD3. joint examination Range of motion The opening measurement routinely obtained is the distance (in millimeters) between the incisal edge of the maxillary central incisors and the incisal edge of the mandibular central incisors when.
Radiographic examination I- Imaging of the TMJ: The goal is to obtain the necessary diagnostic information without unnecessary patient expense or radiation exposure.
Diagnostic Aids and Methods of Investigation I- Imaging of the TMJ: 1-Plain film radiography: • This provides a view of all mineralized tissues “bone”, but can’t show any soft tissue as disc or cartilage. • Limited by superimposition of adjacent structures.
Diagnostic Aids and Methods of Investigation I- Imaging of the TMJ: 2-Conventional tomography: • It produces 3D multiple thin image slices. • true condylar position and reveal osseous changes. • Exposure to radiation is the main disadvantages.
Diagnostic Aids and Methods of Investigation I- Imaging of the TMJ: 3-Panoramic radiography: • show condylar abnormalities such as erosions, sclerosis, resorption, ankylosis, and fractures. • It also gives information about the teeth, mandible, and maxilla, which may help with the overall diagnosis.
Diagnostic Aids and Methods of Investigation I- Imaging of the TMJ: 4-Arthrography: • It involves injection of radiopaque contrast material into the joint spaces. So it can then be visualized.
Diagnostic Aids and Methods of Investigation I- Imaging of the TMJ: 5-Computed tomography/ Cone beam CT: • Newer and faster technique, with a lower radiation dose than conventional whole-body CT. • It provides 3 dimensional thin-slice images on the axial, coronal, and sagittal planes.
Diagnostic Aids and Methods of Investigation I- Imaging of the TMJ: 6-Magnetic resonance imaging: • Detect soft-tissue abnormalities. • Joint and disc can be accurately visualized both at rest and in motion. • Allows for analysis of the blood supply and vascularity of the condyle, detect any pathologic accumulations of fluid within and around the joint. • The main advantage is the complete absence of radiation.
Diagnostic Aids and Methods of Investigation II- Electromyography: • Graphic recording of the electrical potential of muscle. • Used to assess masticatory muscle function in TMD patients. • Shows nocturnal and diurnal parafunctional habits.
Diagnostic Aids and Methods of Investigation III-Ultrasonography: • Sonography is a technique of recording sound waves of high frequency to produce images of the body. • As the sound waves travel through the body, they encounter a boundary between tissues of varying densities.
Diagnostic Aids and Methods of Investigation IV-Mandibular Tracing Devices: • It is used to detect the exact movement of the mandible. • Unfortunately; many disorders create deviations and deflections in mandibular movement pathways. • Therefore, diagnosis should be aided by clinical and radiographic examination.
Diagnostic Aids and Methods of Investigation IIV-Thermography: • Thermography is a technique that records and graphically illustrates surface skin temperatures. • Various temperatures are recorded by different colors, producing a map. • This is not a reliable method, not useful for TMJ diagnosis.
Management of TMJ disorders • The treatment of TMDs must be based on a proper diagnosis, collecting data regarding patient’s history; trauma, accidents, or oral habits. • Management of TMDs can be summarized into supportive and definitive treatments.
Management of TMJ disorders • Supportive therapy; refers to treatment methods that are directed toward altering patient’s symptoms, such as pain and dysfunction. No or little effect on the etiology. • Definitive treatment; directed toward elimination or alteration of the etiologic factors responsible for the disorder.
1- Pharmacological therapy. 2- Physical therapy. . I) supportive therapy
II) Definitive treatment: 1- Occlusal therapy; A-Reversible occlusal therapy. B-Irreversible occlusal therapy 2- Surgery.
I) supportive therapy1- pharmacological therapy • Pharmacologic therapy used to treat symptoms of TMD can be classified into five types: • analgesics • Corticosteroids • muscle relaxants • anti-depressants& anti-anxiety agents • local anesthetics.
I) supportive therapy2- physical therapy • Can be categorized in physical modalities and manual techniques. • Physical therapy Modalities: 1-Thermotherapy: It is the application of hot fomentation on the symptomatic area for 10 to 15 minutes, not exceeding 30 minutes. The primary goal, is to increase blood supply through vasodilatation, leading to decrease pain and joint stiffness.
I) supportive therapy2- physical therapy 2-Coolant therapy: -It is the application of cold fomentation such as ethyl chloride and fluoromethane sprays. -This intend to decrease pain by numbing the symptomatic area. -Combination of hot and cold fomentation is helpful.
I) supportive therapy2- physical therapy 3-Acupuncture: It is one of the alternative Medicine techniques. Its action is still unclear, but was successfully used in treating TMD symptoms.
I) supportive therapy2- physical therapy 4-Electromyographic Biofeedback: some emotional states may be associated to muscle hyperactivity, relaxation training assisted by the use of EMG biofeedback, can reduce diurnal muscle activity; thus reducing pain.
I) supportive therapy2- physical therapy 5-Ultrasound therapy: It has the same concept of thermotherapy, but more effective; because it acts on deeper tissues, not just the surface. Ultrasound not only increases the blood flow in deep tissues but also seems to separate collagen fibers, which improves the flexibility and extensibility of connective tissues, decrease joint stiffness, provide pain relief, improve mobility, and reduce muscle spasm.
I) supportive therapy2- physical therapy 6-Transcutaneous Electrical Nerve Stimulation “TENS”: Electric stimulation devices for treatment of TMD are claimed to have two main purposes; relief of pain and relief of muscle hyperactivity or spasm.
I) supportive therapy2- physical therapy 7-LASER “Light Amplification by Stimulated Emission of Radiation”: It has wide application in dentistry. The only physical risk is eye damage; special eye goggles should be worn for protection.