Download
1 / 35
350 likes | 367 Views
Learn about the complex changes at systemic, organ, and cellular levels in heart failure, as well as evidence-based treatment options. Understand the underlying causes and precipitating factors, and how to optimize therapy for individual patients.

E N D
Optimizing Treatment Of Heart Failure for individual patients By Prof. Mansoor Ahmad FRCP Consultant Cardiologist
Introduction A clinical syndrome characterized by progressive weakening of the heart as a pump, causing complex changes in processes at systemic, organ and cellular levels, finally leading to premature myocardial cell death. This leads to salt and water retention with classical symptoms and physical signs.
Heart failure • Prevalence of symptomatic HF 0.4-2.0%, 6-10% in people over 65 years • Disease of the elderly (mean age > 70 years) • Prevalence is rising • Bad prognosis: 5-year survival rate < 50% • Mortality (even if age adjusted) is increasing Laszlo L. Tornoci,Inst. Pathophysiology,Semmelweis University
Prognosis • Annual mortality rate depends on patients symptoms and LV function • 5% in patients with mild symptoms and mild ↓ in LV function • 30% to 50% in patient with advances LV dysfunction and severe symptoms • 40% – 50% of death is due to SCD
Causes of heart failure • Underlying (true) causes • Precipitating causes (which make the clinical condition worse, ‘decompensate’ the patient)
Underlying causes • Ischemic heart disease • Hypertension • Valvular heart disease • Cardiomyopathies • Other
Precipitating causes 1. Increased workload • Increased cardiac output • metabolic need • (fever, infection, hyperthyroidism) • volume overload • (renal failure, high sodium intake) • Pressure overload • high BP • pulmonary embolism
Precipitating causes 2. Same workload, but weaker heart • Cardiac ischemia • Decreased efficiency (arrhythmias) • Drug effect • Endocarditis, myocarditis
Precipitating causes 3 • Drugs • Non Steroidal Anti Inflammatory Drugs • Steroids • IV fluids • Hydralazine • Beta blockers • Angioedema
Summary of drug therapy *: long term effects are in parentheses
Heart failure • Treatment is evidence based eg. • CONSENSUS 1987 (ACEI) • CHARM 2004 (ARB) • MERIT HF and COPERNICUS (beta blocker)
MERIT-HF and COPERNICUS: Severe Heart Failure Number of Patients to Treat 1 Year in Order to Save One Life • MERIT-HF:13 • COPERNICUS: 15
COPERNICUS Inclusion Criteria Defining Heart Failure EF <0.25 within 6 months prior to randomization Symptoms of dyspnea and/or fatigue at rest or on minimal exertion for at least 2 months No pulmonary rales and no ascites at randomization No or only trace (minimal) oedema of the peripheral limbs at randomization (patients with mild oedema may be enrolled if the oedema is due to a venous disorder)
Heart failure? • Most of the studies use highly selected patients. • On an average 12 to 20% of patients are selected out of total screened. • Where do the rest of the patients fit??
Intolerance to drugs • Approximately 15% withdrawal rate for blocker.
MERIT-HF Severe Heart Failure (NYHA III/IV and EF<0.25) All cause Adverse events Wosening CHF p=0.012 No. of withdrawals p=0.027 p=0.018 66/42 86/62 34/18 Goldstein S et al, JACC 2001;38:932-8
MERIT-HF and COPERNICUS: Severe Heart Failure Yearly Withdrawal Rate of Study Medicine Placebo Meto Δ p-value CR/XL MERIT-HF1 21.7% 15.5% -31% 0.027 COPERNICUS 18.5% 14.8% -23% 0.02 Goldstein S et al, JACC 2001;38:932-8 Packer et al, NEJM 2001;344:1651-8
Heart failure • A variety of patients are seen in day to day practice who will not fit completely for the prescribed GUIDELINES.
Blood Pressure levels • Patients with low Blood Pressure levels tend to tolerate ACE inhibitor, Angiotensin Receptor Blocker and blocker less well.
MERIT-HF Severe Heart Failure (NYHA III/IV and EF<0.25) Baseline Blood Pressure and Heart Rate Variable Placebo Meto CR/XL n=396 n=399 Systolic blood pressure 124 125 Diastolic blood pressure 77 77 Heart rate 85 85 Goldstein S et al, JACC 2001;38:932-8
MERIT-HF and COPERNICUS: Severe Heart Failure Baseline Blood Pressure and Heart Rate MERIT-HF1 COPERNICUS Variable Placebo Meto CR/XL Placebo Carvedilol n=396 n=399 n=1133 n=1156 SBP 124 125 123 123 DBP 77 77 76 76 HR 85 85 80 80
Chronic Obstructive Airway Disease blocker
Chronic kidney disease • Caution with ACE inhibitor and Angiotensin Receptor Blocker. • BP control
Hyperkalemia • Hyperkalemia is the commonest reason for temporary pacing. • ACE inhibitor • Angiotensin Receptor Blocker • Spiranolactone • Possibly blocker.
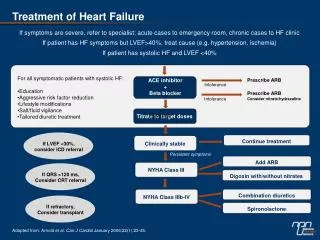
Heart failure • Maintain symptomatic control • Control fluid retension • Use diuretics • Serum potassium.
Heart failure • Add ACE inhibitors/ Angiotensin Receptor blocker early • Build up the dose over weeks if blood pressure is low • Watch out for • cough (upto 20%) • Serum potassium • Serum creatinine
Heart failure • Add beta blocker after the fluid overload is controlled • Build up the dose slowly • Watch out for brochospasm, worsening failure??
Heart failure • Use digoxin appropriately and cautiously • Main indication is Fast Atrial Fibrillation with failure • Serum potassium • Toxicity
DIAL: Randomized Trial of Telephonic Intervention in Chronic Heart Failure
DIAL: primary endpoint: all-cause mortality/heart failure hospitalizations
Summary • Tailor treatment to individual needs of thepatients • Dosage to tolerability levels • Support care as much as possible • Advise on possible precipitating factors eg. Flu vaccination in autumn for COAD patients
Summary • Treat cause whenever possible eg. Revascularization, Valve replacement. • Control arrythmias • Close watch on patients even if they are well, as Sudden Cardiac Death is common in all • CRT and ICD in appropriate cases (both clinical and financial) • Transplant • Artificial heart