Download
1 / 32
320 likes | 334 Views
This presentation by Professor Christopher R. Burton and Noreen Edwards explores a layered perspective on co-production in stroke care, addressing key challenges, solutions, and a case study on end-of-life care in a co-production context. The prudent principles of co-production, outcomes focus, and broader perspectives on collaborative knowledge sharing are discussed, emphasizing the role of stakeholders in achieving health outcomes. The presentation delves into the diverse layers of knowledge in the stroke system, including evidence from research, professional wisdom, service user experience, and embedded and local knowledge. It analyzes gaps in knowledge translation and proposes a new lens on co-production for enhancing healthcare practices.

E N D
A Layered approach toco-production around stroke Professor Christopher R Burton Noreen Edwards Chair of Rehabilitation and Nursing Research Improvement science fellow, Health foundation
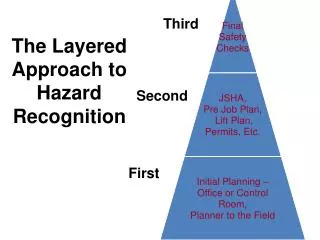
Presentation overview • Setting some co-ordinates • Where is ‘knowledge’ in the stroke system? • Co-production: a ‘layered’ perspective • Some key challenges and potential solutions • Case study: stroke and end-of-life care
CO-PRODUCTION Closer to home • Prudent Healthcare • “achieve health and wellbeing with the public, patients and professionals as equal partners through co-production” • Co-production … enables citizens and professionals to share power and work together in equal partnership, creating opportunities for people to access support when they need it and to contribute to social change.
Prudent Principles of co-production • Value all participants as equals and assets • Everyone has a contribution to make, whether as experts through experience or experts through training. We should acknowledge this in everything we do, and build from our strengths. • Develop and support peer networks • Social capital – networks of friendship and support – are vital to our health and well-being. Peer networks help to build confidence and give people a voice, and the opportunity to help others. • Reciprocity • The impulse to give back is universal. Wherever possible, we must replace one-way acts of largesse with two-way transactions. ‘You need me’ becomes ‘We need each other’. • Outcomes focus • The focus of co-production is on achieving the outcomes that matter to individuals, rather than on the process of delivering services. The role of the professional is to facilitate that journey.
Broadening our perspective ‘…the collaborative process of bringing a plurality of knowledge sources and types together to address a defined problem and build an integrated or systems-oriented understanding of that problem.’ Armitageet al. (2011)
The “stroke system” • Mix of generalist and stroke specialist services, located within wider complex systems of people, teams, organisations and sectors • Diverse stakeholder group with varying degrees of ‘focus’ on stroke • Bench and applied research programmes • Patient focused research priorities / expectations about involvement in research • Across research programmes (e.g. HTA / HSD&R) and infrastructure (e.g. CLAHRCs) • National Clinical Guidelines • National Improvement Programmes • Protocols / care bundles • Audit and feedback mechanisms • Project or initiative related
What ‘knowledge’ is in the stroke system? EVIDENCE FROM RESEARCH PROFESSIONAL WISDOM SERVICE USER EXPERIENCE EMBEDDED KNOWLEDGE PERFORMANCE KNOWLEDGE LOCAL KNOWLEDGE
‘traditional’ layers of Co-production • Individual • Evidence-based practice • Shared decision-making • Service • Experience-based co-design
Decision aids Available for a number of issues, such as: • Statins • Anticoagulants, Atrial Fibrillation and Stroke Prevention
Generating knowledge of what works in stroke services
Closing the gap between ‘what we know’ and ‘what we practice’
Gaps in knowledge Translation? • GAP 1: from the bench to bedside , or the process of transferring basic science knowledge into new drugs and technologies. • GAP 2: is the process of taking current scientific knowledge and ensuring it is applied routinely in practice. Woolf SH: The Meaning of Translational Research and Why it Matters. JAMA 2008, 299:211-213 .
Traditional & historical view • Focus on individual (behaviour) • Skilling practitioners up • As ‘rational actors’ that can perform ‘evidence-based practice’ • Evidence as a product (e.g. guideline), which has common meaning • Linear – logical view of evidence use (push): • researchers publication practitioners • Lack of consideration of the influence of context of practice/service delivery) (pull)
Knowledge Creation Knowledge validation Knowledge Dissemination Knowledge adoption Two communities Researchers Users Research priorities Nutley et al 2000; 2008
In reality… • Research is only one source of information used for practice and service delivery • It gets transformed – individually and/or collectively [or can often be ignored] • Viewed differently by individuals & groups • Action occurs in social and organisational structures – which can be more or less facilitative – context is KEY! • i.e. implementation is not a one-off event
A NEW LENS ON CO-PRODUCTION? • “A systematic and interdisciplinary approach to sustained engagement with stakeholders, and their systems, in generating implementable knowledge with impact in healthcare and health” • The assumption is that knowledge of how to improve healthcare is more likely to have impact if: it addresses stakeholder concerns; is synergistic with conceptual and other frameworks that are prevalent within relevant systems; is recognised as valuable and credible; and is mobilised in creative and sustained ways throughout encounters between stakeholders.
Working together in the knowledge system? • Ontological and Epistemological differences • Professional, organisational and other incentives • Moving from consultation, through collaboration, towards partnership • Who are the key stakeholders? • Understanding stakeholder perspectives / systems / contexts • Where do stakeholder perspectives come together? • What do different stakeholders bring to the table? • Should different stakeholder perspectives be integrated? • How should we embed implementation across the ‘knowledge endeavour’? • What are the skills required to facilitate this ‘knowledge endeavour’?
Aims of the study • To identify patterns of dying in acute stroke services • To explore patient and family carer experiences • To explore clinical decision-making around end of life care in acute stroke
Design issues • Stakeholder perspectives • Service user • Patient • Family carers • Professionals • Different professional groups Mixed methods design: • Observational study • Biographical, clinical and service data were collected from consecutive admissions to four UK acute stroke services over a 6-month period • Dying trajectories classified as sudden, rapid, episodic, slow decline or other • Interviews • With patients, family carers and bereaved relatives • Think-aloud study • With members of the multi-disciplinary team
Interviews with patients and families • Paying attention to clinical geography, and resonance with information giving • Honesty is the best policy, with displayed compassion and concern • Formalising information-giving through technologies or systems • Considerable ‘forgiveness’ for system problems
What were staff thinking about? • Developing an understanding, or ‘mental model’ of what is happening to the patient • The level of involvement to have in the patient’s care • What additional information to seek, or investigations to make (if any) • Establishing parameters for the escalation of active intervention / ceilings of care • Commencing best interest / advance directive / palliative care / end of life care discussions with families
Thinking processes The overarching ‘thinking’ processes uncovered in our data were: • Evaluating signs and symptoms • Seeking more information by completing more investigations • Seeking the views of others and confirmation of decisions through peers, members of the team and family members • Drawing on personal resources of clinical experience • Putting things into an individual context, by focusing on the patient’s pre-stroke life, wishes and preferences • Placing the self within the context of the decision • Looking to the future considering the potentiality of death and possible future scenarios
Impacts of co-production • Greater understanding (and sharing) of the perspectives of different stakeholders • Communication around end of life issues / permission • Rejecting the notion of the ‘good death’ • Acknowledgment of the emotional work of palliative and end of life care • Identification of a middle-ground / approach to practice between research, professionals and service users • “We can plan for the worst, but hope for the best” • Service improvement and research challenges • The development and testing of strategies that support implementation of this approach to palliative care practice
acknowledgements Funders of research projects referred to in this presentation • Health Foundation • Marie Curie Cancer Care • Health Care Research Wales • National Institute for Health Research Stakeholders who have engaged in these studies. For further information: c.burton@bangor.ac.uk @chrisburton5