Download
1 / 22
300 likes | 1.27k Views
Usual and Unusual Imaging Findings and Pitfalls in Cerebral Venous Sinus Thrombosis Toshio Moritani, Wendy RK Smoker, Dawson Wolfe, Theodore Donta, Bruno A Policeni, Bakhshandeh Pour,Gholamreza, Jack Kademian, Ho Kyu Lee, Yutaka Sato

E N D
Usual and Unusual Imaging Findings and Pitfalls in Cerebral Venous Sinus Thrombosis Toshio Moritani, Wendy RK Smoker, Dawson Wolfe, Theodore Donta, Bruno A Policeni, Bakhshandeh Pour,Gholamreza,Jack Kademian, Ho Kyu Lee, Yutaka Sato Department of Radiology, University of Iowa Hospitals & Clinics
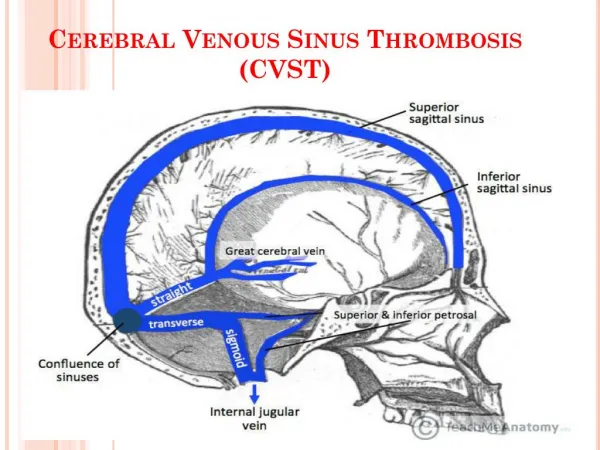
Introduction The diagnosis of cerebral venous sinus thrombosis (CVST) is difficult because presenting clinical symptoms are often non-specific such as headache, fever, seizure, numbness, weakness, ataxia and mental status changes. There are also a variety of predisposing factors and associated disease conditions, such as pregnancy, oral contraceptives or other medications, various infections (mastoiditis, sinusitis, meningitis), extrinsic compression or local invasion by tumor, hypercoagulopathies (protein C, S, or Factor V deficiencies, etc), nephrosis, dehydration, and drug abuse. CVST causes pulmonary embolism. Imaging findings are also complex because there are different phases of thrombosis at the different anatomical locations, with or without parenchymal abnormalities such as venous ischemia and hemorrhage.
We reviewed the clinical information and imaging studies of 50 patients with documented CVST. Imaging modalities included CT, MRI (T1WI, T2WI, FLAIR, gadolinium enhanced T1WI, gradient echo T2* and diffusion-weighted images (DWI)), MR venography (3D dynamic contrast-enhanced, 3D contrast-enhanced time-of-flight (TOF), 2D TOF, 2D phase contrast), and conventional angiography/venography. The purpose of this exhibit is to demonstrate usual and unusual findings of cerebral CVST and diagnostic pitfalls.
CT CT is usually performed as the first line investigation on an emergency basis. CT values of acute or subacute thrombi on non contrast CT are around 70 HU (Fig 4). However, it is often difficult to detect thrombi because of the wide range of values in acute to chronic phase thrombi and in the normal venous sinuses with different conditions (dehydration, polycythemia, antacid medication, previous contrast, surrounding parenchymal edema, etc), and artifacts. It is also difficult to detect thrombi on contrast enhanced CT, usually seen as a defect in the venous sinus (empty delta sign) for the same reasons (Fig 2). CT demonstrates venous ischemia as low density areas (Fig 5), CT is useful for detecting subdural, subarachnoid,and intraparenchymal hemorrhages, as well as hemorrhagic infarction associated with CVST (Figs 7, 12 and 17).
MRI T1 and T2-weighted images (T1WI,T2WI) and FLAIR Acute phase thrombi (within 72 hrs) are usually shown as isointense on T1WI (Figs 1, 4, 5, 12, and 14) and hypointense on T2WI and FLAIR, thus difficult to differentiate from normal veins. Hyperintense thrombi (met Hb) on T1WI are usually seen in the subacute phase (after 3-5 days) (Figs 1, 4, 5, 8, 13, 15-17). During the subacute to chronic phase, T2WI shows thrombi as mixed hypo- and hyperintensity (Figs 7 and 8), and then it turns hyperintense (Figs 8 and 9). TIWI continue to show hyperintensity of thrombi in the subacute to early chronic phase. However, the T1 signal again turns isointense during the chronic phase (Figs 8 and 9). It is often difficult to detect chronic thrombus itself with venous sinus stenosis / occlusion on MRI (Figs 10 and 11). The only abnormalities may be dilated collateral veins.
Gradient echo T2* (GRE) images Normal venous sinuses and veins are usually iso or mildly hyperintense on GRE at 1.5T. GRE is very useful in early detection of acute to subacute thrombi seen as very low signal (deoxy Hb) (Figs 1, 2, 5, 6, and 12), especially before T1WI show high signal in the thrombi. GRE can clearly visualize acute/subacute thrombi as areas of low signal in small venous branches, such as the deep venous system (Fig 1), vein of Labbe (Fig 2) and cortical veins (Fig 5). GRE can also detect hemorrhage associated with venous ischemia or dural arteriovenous fistulae. However, GRE often misses late subacute and chronic phase thrombi which are shown as isointense or high signal on GRE (Figs 8 and 9). GRE images on 3T demonstrate venous structures as low signal flow voids (Fig 3). It can be difficult to identify thrombi on GRE at 3T.
Diffusion-weighted images (DWI) In venous ischemia, venous occlusion leads to retrograde venous pressure causing BBB breakdown with leakage of fluid, first resulting in vasogenic edema. This is followed by decreased cerebral perfusion pressure and flow resulting in cytotoxic edema. DWI can differentiate between vasogenic and cytotoxic edema (Fig 4, 5, 11, and 15). DWI shows vasogenic edema as mildly hypo- or hyperintense with increased ADC and cytotoxic edema as hyperintense with decreased ADC. Areas with restricted diffusion and decreased ADC often result in infarction. DWI shows subacute phase thrombi as hyperintense with decreased ADC (Fig 8). Diffusion restriction of thrombi may be predictive of a low rate of recanalization. DWI also can show pyogenic abscesses / pus collections (Fig 9) or cholesteatomas as hyperintense lesions with decreased ADC.
Post-contrast T1-weighted images (Gd-T1) Acute and subacute thrombi are usually seen as defects in the enhancing venous sinus (Fig 2, 5, 7, 8, and 13). It is occasionally difficult to evaluate the presence of thrombi on Gd-T1WI because flow voids can be seen in the enhancing venous sinuses or thrombi may be small and located in venous branches (Fig 5). Chronic phase thrombi often enhance and can appear similar to normal enhancing venous sinuses (Fig 8). Dural enhancement (Fig 2) and leptomeningeal enhancement (Fig 5) are often seen in association with CVST. In chronic CVST, visualization of collateral veins may be a clue to the diagnosis (Figs 10 and 11).
MR venography (MRV) and conventional angiography On MRV, venous sinus occlusion or stenosis associated with CVST is sometimes difficult to differentiate from normal anatomic venous variants such as hypoplasias or aplasias (Fig 5). Dynamic contrast-enhanced 3D MRV (DC 3DMRV) is better for visualization of venous sinus structures, especially their branches, than 2D, 3D TOF, or 2D PC MRV (Figs 2, 7, and 11). If the thrombus has high signal intensity onT1WI (subacute phase) or enhances on Gd-T1WI (chronic phase), DC 3DMRV may be falsely negative for the presence of thrombi (Figs 1 and 8). Only conventional angiography shows small arteriovenous fistula (Fig 6).
Fig 1. Acute to early subacute transverse sinus and deep venous systemthrombosis FLAIR GRE GRE T2WI T1WIs DC 3DMRV 4 day follow-up after full dose heparin-GRE images 35-year-old female smoker on oral contraceptives with severe headache. GRE clearly shows thrombus as very hypointense in theright transverse sinus compared tothe normal side(iso or mildly hyperintense), with extension intothe straight sinus,vein of Galen, right internal cerebral vein, right thalamostriate vein, and medullary veins. On T2 and T1WIs, these thrombi are hard to detect. There is non-visualization of the straight sinus, vein of Galen and right transverse sinus on the DC 3DMR. Four day follow-up MRI shows evolution of the thrombus, with GRE now less hypointense, and T1WI showing more obvious hyperintensity in theright transverse and straight sinuses.On follow-up MRVthe straight and righttransverse sinusesare visualized, but this is mainly due to the high T1 thrombus itself because MRV is essentially a T1-weighted image. T2 GdT1 T2 4 year follow-up MRI GdT1
GRE Gd -T1WI 2D TOF MRV Fig 3. Normal venous sinus on 3T Fig 2. Acute thrombosis in the transverse sinus extending into vein of Labbe T2WI GRE DC 3D MRV 35 year-old male with paranoid schizophrenia.Only GRE can demonstrate thrombus in theleft transverse sinus and the venous brancheswith extension into thevein of Labbe. Gd T1WI shows meningeal and dural enhancement associated with venous engorgement. 2DTOF MRV shows non-visualization of the left transverse, sigmoid sinus and jugular vein. DC 3DMRV shows morevisualization of venous branches (occlusion of vein of Labbe) and collaterals although there is arterial contamination. 42 year-old female.On 3T MRI, T2WIclearly shows low signal inthe normal transverse sinus.GRE also shows low signal in thenormal transverse sinus and branches. GRE on 1.5 T appears more useful for depicting acute thrombus than 3T.
Fig 4. Acute and early subacute thrombus in the transverse sinus and vein of Labbe, extending into the deep venous system with progression of venous infarction DWI T1WI CT T2WI 57 year-old man with dysarthria. Non-contrast CT 24 hrs from onset of symptoms shows thrombus in the left transverse sinus as hyperdense. T2WI shows venous ischemia in the left temporal lobe. DWI shows mild restriction with increased ADC (not shown), representingvasogenic edemadue to venous ischemia. Sagittal T1WI showsleft transverse sinusthrombosisas isointense at this time. 3 day follow-up with mental status changes. Progressive symptoms with mental status changes. Three day follow-up MRI shows progression of ischemia in the basal ganglia and thalamus. DWI shows high signal with some decreased ADC areas (not shown), representingcytotoxic edema.Sagittal T1WI shows extension of hyperintensethrombosis of the transverse sinus extending into the deep venous system.
Fig 5. Superior sagittal sinus and cortical vein acute thrombosis with venous jnfarcts T2 GdT1 a T1WI MRV GRE T2WI CT DWI GdT1s ADC GRE 23 year-old hypercoagulable male with a history of partial complex seizures. Now complains of headache and left-sided weakness. MRI/MRV obtained 4 days after onset of symptoms. CT shows venous ischemic lesions as low density but thrombus is not visualized. On GRE, hypointense lesions in an arborizing pattern are noted in thecortical veinsof the frontal lobes. On T2 and pre/post-contrast T1WIs, the thrombus is not well-visualized. DWI demonstrates hyperintense lesions with decreased ADC (cytotoxicedema) and surrounding increased ADC (vasogenic edema) consistent with venous infarcts. Axial and coronal Gd T1WIs shows leptomeningeal enhancement. Dynamic contrast 3D MRV reveals non visualization of theanterior 2/3 of the superior sagittal sinus and cortical veins. Coronal MRV shows that the left transverse and sigmoid sinuses and internal jugular vein are hypoplastic. This isnormal venous sinus variation. MRI, including GRE, shows no evidence of thrombus in the left transverse sinus. Looking only at the MRV, the diagnosis of sinus thombosis is often difficult. Conventional MRI, including GRE and DWI, is essential for making the correct diagnosis.
Fig 6. Left transverse sinus acute thrombosisand right cerebellar hemorrhage due to dural AV fistula Angiogram MRV CT T2WI GRE 39 year-old female with sudden onset of headache and vertigo. CT, T2WI and GRE show a right cerebellar hemorrhage. Only GRE demonstrates acute thrombus in theleft transverse sinus. Coronal view of dynamic contrast 3D MRV shows a defect in theleft transverse sinus. MRV could not demonstrate the small dural AV fistula, seen on the conventional angiogram following selective injection of the right posterior meningeal artery. Fig 7. Acute to subacute left internal jugular vein and sigmoid sinus thrombosis 2D TOF MRV T2WI T1WI GdT1 2D PC MRV 5 year-old girl with acute mastoiditis.The T2WI shows the left mastoid fluid collection as high signal intensity, and thrombus aslow signal in the left jugular foramenand high signal in the sigmoid sinus.. The T1WI shows thrombus isointensity. GdT1 shows the defects with surrounding sinus and left mastoid enhancement. 2D PC and 2DTOF MRV demonstrates non-visualization of the left sigmoid sinus and internal jugular vein. The 2D TOF MRV shows better visualization of venous branches than that seen on the 2D PC MRV. GRE
Fig 8. Subacute to chronic phase thrombosis in the left jugular vein, transverse and sigmoid sinuses 3 weeks after surgery DWI ADC T1WI GdT1 GRE T2WI 4 months after surgery MRV 7 year-old boy with headache and diplopia two weeks following decompression surgery for a high-riding jugular bulb.. T2 and T1WIs show subacute phase thrombus in theleft transverse and sigmoid sinuses extending from the left jugular bulbas hyperintense, with peripheral enhancement on Gd-T1WI. GRE showspartially low and partially isointense signal in the subacute thrombusof the left transverse sinus. DWI shows thesubacute thrombusas hyperintense with decreased ADC. Follow-up MRI 4 months after surgery shows thechronic phase thrombusas hyperintense on the T2 and isointense on the T1WI, with marked enhancement. GRE shows thechronic phase thrombus as isointense. Dynamic contrast 3D MRV shows non-visualization of theleft jugular bulb and internal jugular vein. Theleft transverse and sigmoid sinusesare visualized but this may represent thrombus enhancement.
Fig 9. Subacute to chronic phase thrombosis in the right jugular vein and sigmoid sinus T2WI T1WI GdT1 GRE DWI ADC 54 year-old male with mastoid abscess..T2WI shows rightexpansile mastoid fluid collectionandthrombus as high signal in the jugular foramen and sigmoid sinus. The T1WI shows isointensity. Gd T1WI shows marked rim enhancement and left mastoid enhancement. GRE shows isointense thrombus. DWI shows very high signal with decreased ADC in the right mastoid and sigmoid sinus area, consistent with abscess. At surgery the wall of the sigmoid sinus was disrupted with pus and thrombus formation. Fig 10. Chronic phase thrombosis in the superior sagittal sinus and collateral veins T1WIs GdT1 3D TOF MRV DC 3D MRV Angiogram 52 year-old female with Factor V coagulopathy, presenting with chronic headache and new onset of seizures.. MRI could not detect any definite venous sinus thrombus or stenosis /occlusion. However, it does shows collateral veins secondary to venous sinus stenosis. T1WIs showdilated medullary veins. Gd-T1WI showsa dilated tortuous Basal vein of Rosenthalas a collateral. 3D TOF MRV, dynamic contrast 3D MRV, and cerebral angiography show stenosis of the superior sagittal sinus and multiple collateral veins.
Fig 11. Chronic phase thrombosis in the jugular vein, sigmoid and the superior sagittal sinuses, and collateral veins. T2WI T1WI GRE MRV FLAIR DWI ADC Gd-T1WIs 64 year-old female with recurrent strokes for 2 years, presenting with new onset of hand numbness and balance problem. T2, T1, and GRE images show hyperintanse chronic phase thrombus in theleft jugular vein and sigmoid sinus. Dynamic contrast 3D MRV shows non-visualization of the left jugular vein and sigmoid sinus, andsevere stenosis or occlusion in the superior sagittal sinus. FLAIR shows multiple hyperintense lesions in the bilateral frontal white matter and cortex. DWI shows these lesions as iso or hyperintense with increased ADC, consistent with vasogenic edema due to venous ischemia. A hemorrhagic focus is also noted on DWI. Axial Gd-T1WIs revealenhancing dilated medullary veinsas collaterals secondary to chronic superior sagittal sinus stenosis/occlusion. Sagittal Gd-T1 shows enhancement of the superior sagittal sinus which may represent chronic phase thrombus. It is very difficult to detectchronic phase thrombus in the superior sagittal sinus on MRI.
Fig 12. Early subacute phase thrombosis in the right jugular bulb, sigmoid, and transverse sinuses through the superior sagittal sinus CT CT T1WIs GRE Gd-T1WI GRE T2WI 39 year-old female with a history of head trauma and jugular foramen fracture. CT shows multiple brain contusions in the right temporal lobe and bilateral frontal lobes andasmall subdural hematomaadjacent to the torcula.. However, it is hard to detect the thrombus. CT of the temporal bone shows fractures involving theright jugular foramen. GRE clearly shows hypointense acute thrombus in theright transverse sinus.Gd-T1WI shows the transverse sinus thrombus as a defect. Another GRE showssagittal sinus thrombosisand hemorrhagic contusions in the right temporal lobe as low signal. On the T2WI, thrombus is low signal but similar to the normal flow void in the venous sinus. Sagitttal T1WIs demonstrate superior sagittal sinus thrombosisas iso or mildly hyperintense, and thesmall subdural hematomaas hyperintense signal. a b T1
Fig 13. Subacute phase thrombus in the superior sagittal sinus with associated hemorrhage. 57 year-old female with invasive glioblastoma multifome.FLAIR shows hemorrhagic masses with surrounding edema in the occipital lobes bilaterally. Sagittal Gd-T1WI shows enhancing tumor invading the superior sagittal sinus causing thrombosis. Sagittal T1WI shows superior sagittal sinus thrombosis as hyperintense, consistent withsubacute phase thrombus. T1WI FLAIR Gd-T1WI Fig 14. Acute phase thrombosis in the superior sagittal sinus after surgery for vestibular schwannoma resulting in extensive pulmonary embolism and MCA embolus, presumably via a patent foramen ovale. Perfusion Ventilation T2WI Angiogram T1WI 72 year-old male with mental status changes and respiratory failure after surgery. Sagittal T1WI showsacute isointense thrombusin the superior sagittal sinus 24 hrs after surgery. Pulmonary perfusion scan shows multiple perfusion defects in the lower lungs fields bilaterally which are mismatched with the ventilation scan. T2WI shows right MCA infarction. Angiogram demonstrates anembolic stenosisin the right MCA.
Fig 15. Isolated deep venous system thrombosis with hemorrhage in the choroid plexus bilaterally. T1WI T2WI GRE DWI ADC 5 day-old boy with bacterial meningitis.The T1WI shows hyperintense thrombus in the internal cerebral veins and their branches.. Hemorrhage in the choroid plexi is hyperintense on the T1WI and hypointense on the T2WI. Small T1 hyperintensepetechial hemorrhagesare seen in the frontal white matter bilaterally due to venous ischemia. Coronal GRE demonstrates the thrombias hypointense. DWI shows vasogenic edema in the bilateral frontal white matter as hypointense with increased ADC and hemorrhage in the choroid plexi as hyperintensewith decreased ADC.
Fig 16. Extensive thrombosis in the superior sagittal sinus and deep venous system. 4 month-old boy with shaken baby syndrome.T1WI shows extensive thrombus in the superior sagittal sinus, occipital sinus and deep venous system. T1 and T2WIs show bilateral subdural fluid collections and an old contusion in the right frontal cortex. T2WI T1WIs W Fig 17. Extensive thrombosis of the superior sagittal sinus and deep venous system with thalamic hemorrhage. CT T1WI T2WIs Ultrasound 7 day-old boy with congenital nephrosis syndrome of the Finnish type. CT demonstrates bilateral thalamic hemorrhages and hyperdense thrombus in the sagittal sinus, straight sinus, and deep venous system. The sagittal T1WI shows extensive hyperintense thrombus in the superior and inferior sagittal sinuses, straight sinus, and deep venous system that are very hypointense on the T2WI . Ultrasound shows a large hyperechoic kidney consistent with congenital nephrosis.
References • 1.Fellner FA, et al.Importance of T2*-weighted gradient-echo MRI for diagnosis of cortical vein thrombosis. Eur J Radiol 2005;56:235-239 • Idbaih A, et al. MRI of clot in cerebral venous thrombosis: High diagnostic value of susceptibility-weighted Images. Stroke 2006;37:991-995 • Selim M, et al. Diagnosis of cerebral venous thrombosis with echo-planar T2*-weighted magnetic resonance imaging. Arch Neurol 2002;59(6):1021-1026 • Hinman JM, et al. Hypointense thrombus on T2-weighted MR imaging: a potential pitfall in the diagnosis of dural sinus thrombosis. Eur J Radiol 2002;41(2):147-152 • Lovblad KO, et al. Fast contrast-enhanced MR whole-brain venography. Neuroradiology 2002;44(8):681-688 • Cakmak S, et al. T2*SW-weighted MRI in cortical venous thrombosis. Neurology 2004;63:1698 • Duncan IC, et al. Imaging of cerebral isolated cortical vein thrombosis. AJR Am J Roentgenol 2005;184:1317-1319 • Shah VA, et al. Cerebral venous sinus thrombosis following jugular bulb decompression. Semin Ophthalmol 2006; 21:41-44. • Canhao P, et al. Causes and predictors of death in cerebral venous thrombosis. Stroke 2005;36:1720-1725 • Cakmak S. et al. Pulmonary embolism: An unusual complication of cerebral venous thrombosis. Neurology 2005;65:1136-7. • Favrole P, et al. Diffusion-weighted imaging of intravascular clots in cerebral venous thrombosis. Stroke 2004;35:99-103.