Download
1 / 25
290 likes | 578 Views
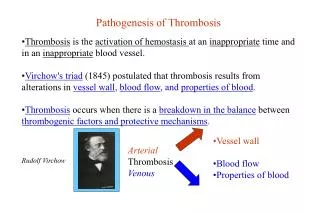
Overview of Thrombosis . •Bleeding disorders are relatively rare , thrombosis is a common medical disorder recognized for over 100 years. • Intravascular thrombosis and embolism are common clinical manifestations of many diseases.

E N D
Overview of Thrombosis •Bleeding disorders are relatively rare, thrombosis is a common medical disorder recognized for over 100 years. •Intravascular thrombosis and embolism are common clinical manifestations of many diseases. •Normal hemostasis limits blood loss by regulated interactions between the vessel wall, platelets, and plasma proteins. •Unregulated activation of coagulation causes thrombosis, which reduces blood flow to organs like brain and myocardium.
Overview of Thrombosis (cont’d) •Certain patient groups are particularly prone to thrombosis: --immobilized after surgery; --chronic congestive heart failure; --atherosclerotic vascular disease; --malignancy; or --pregnant.
Overview of Thrombosis (cont’d) •Many of these "thrombosis-prone" patients have no identifiable hemostatic disorder. •Certain groups have an inherited "hypercoagulable"(thrombophilia) or "prethrombotic" state that predisposes them to thrombosis. •Prethrombotic patient can be identified: --repeated episodes of thromboembolism without an obvious predisposing condition; --family historyof thrombosis; and --well-documented thromboembolism in adolescents/young adults.
Overview of Thrombosis (cont’d) •No clinically useful screening tests for the prethrombotic state. •Several of the inherited prethrombotic disorders can be diagnosed with specific immunologic and functional assays.
Overview of Thrombosis (cont’d) •These coagulation reactions are regulated by: --antithrombin, which forms complexes with all coagulation protein serine proteases except factor VII; and --by the thrombomodulin-protein C-protein S system, which inactivates factors Va and VIIIa.
Inhibitors of Blood Coagulation •Coagulation is a multifactorial pathway of "accelerators". •Coagulation is tightly regulated and only a small quantity of each coagulation enzyme is converted to its active form. •Regulation is important- there is enough clotting potential in 1 mL of blood to clot all the fibrinogen in the body in 10 to 15 s! •Blood fluidity is maintained by the following properties: --flow of blood itself; --adsorption of coagulation factors to surfaces; and --by the presence of multiple inhibitors in plasma.
Inhibitors of Blood Coagulation (cont’d) •These inhibitors have distinct modes of action: --tissue factor pathway inhibitor (TFPI); --antithrombin; --protein C system; and --fibrinolysis.
Inhibitors of Blood Coagulation (cont’d) Antithrombin: •Antithrombin forms "complexes" with all the serine protease coagulation factors except factor VII, this "kills" the protease. •Rates of complex formation are "accelerated" by heparin and heparin-like molecules on the surface of the endothelial cells. •This ability of heparin to accelerate the activity of antithrombin is the basis for heparin's action as a potent anticoagulant.
Inhibitors of Blood Coagulation (cont’d) Protein C System: •Protein C is converted to an active protease by thrombin after it is bound to an endothelial cell protein called thrombomodulin. •Activated protein C then inactivates cofactors V and VIII by proteolysis, which slows down two critical coagulation reactions. •The inhibitory function of protein C is enhanced by protein S.
Inhibitors of Blood Coagulation (cont’d) Protein C System: •Protein C is converted to an active protease by thrombin after it is bound to an endothelial cell protein called thrombomodulin. •Activated protein C then inactivates cofactors V and VIII by proteolysis, which slows down two critical coagulation reactions. •The inhibitory function of protein C is enhanced by protein S.
Inhibitors of Blood Coagulation (cont’d) Fibrinolysis: •Clot lysis and vessel repair begins immediately after the formation of the definitive hemostatic plug. •Tissue plasminogen activator (tPA) and urokinase (uPA), diffuse from endothelial cells and convert plasminogen, adsorbed to the fibrin clot, into plasmin. •Plasmin then degrades fibrin polymer into small fragments. •tPA and uPA are regulated by plasminogen activator inhibitor-1 (PAI-1); plasmin is regulated by a2-plasmin inhibitor (a2-PI).
Pathophysiology of Thrombosis •Reduced levels/dysfunctional forms of antithrombin or proteins C and S result in a “hypercoagulable” or prethrombotic state. •Description of blood coagulation implies that the process is uniform throughout the body, it's not. •Hemostatic plugs in veins where blood flow is slow are rich in fibrin and trapped RBC's and contain relatively few platelets. •Venous thrombi are often called red thrombi because of their appearance in surgical and pathologic specimens. •The friable ends of these red thrombi, which often form in leg veins, can break off and embolize to the pulmonary circulation.
Pathophysiology of Thrombosis (cont’d) •Conversely, thrombi that form in arteries under high flow are predominantly composed of platelets and have little fibrin. •These are termed white thrombi, and may readily dislodge from the arterial wall and embolize to distant sites, causing ischemia. •These thrombi are a particularly common cause of embolism in the cerebral and retinal circulation. •Most myocardial infarctions are due to thrombi that form after rupture of atherosclerotic plaques in diseased coronary arteries.
Pathophysiology of Thrombosis (cont’d) •There is little difference between hemostatic plugs, which are a physiologic response to injury, and pathologic thrombi. •To underscore the similarity, thrombosis has been described as coagulation occurring in the wrong place or at the wrong time.
This is the microscopic appearance of a pulmonary embolus (PE) in a major pulmonary artery branch. Here is a large pulmonary thromboembolus seen in cross section of this lung. The typical source for such thromboemboli is from large veins in the legs and pelvis.
This pulmonary thromboembolus is occluding the main pulmonary artery. Persons who are immobilized for weeks are at greatest risk. The patient can experience sudden onset of shortness of breath. Death may occur within minutes. The main pulmonary trunk and pulmonary arteries to right and left lungs are seen here opened to reveal a large "saddle"pulmonary thromboembolus. Such an embolus will kill your patient.
Overview of Approach to Treatment •Prevention and treatment of thromboembolic disease differs depending on whether it involves venous or arterial circulation. •Venous thrombosis can be effectively prevented: --by reducing the coagulability of blood, --by reducing venous stasis, or --by rendering fibrin more susceptible to fibrinolysis. •The objective of treating venous thrombosis are: --to prevent local extension of the thrombus, --to prevent the thrombus from embolizing, and --to induce accelerated fibrinolysis.
Overview of Approach to Treatment (cont’d) Drugs of choice: --Heparin; --Warfarin (coumarin derivatives); --Fibrinolytic enzymes (e.g., tissue plasminogen activator).
Overview of Approach to Treatment (cont’d) •Heparin is a complex sulfated-polysaccharidetermed a glycosaminoglycan: --Heparin, which is injected, reacts with antithrombin and enables it to rapidly inhibit most coagulation proteases, especially thrombin and factor Xa.
Overview of Approach to Treatment (cont’d) •Warfarin prevents the reduction of vitamin K epoxides in liver microsomes and induce a state analogous to vitamin K deficiency. •It slows clot formation by impairing the biologic activity of the prothrombin complex proteins and is used to prevent the recurrence of venous thrombosis and pulmonary embolism. •Given orally.
Anticoagulant and Fibrinolytic Therapy • Anticoagulation with heparin, followed by treatment with oral vitamin K antagonists, is the standard treatment for acute venous thrombosis and pulmonary embolism. •Chronic oral anticoagulation is used to prevent cerebral arterial embolism from cardiac sources or from atherosclerotic arteries. •These agents retard fibrin deposition on established thrombi and prevent the formation of new thrombi.
Anticoagulant and Fibrinolytic Therapy (cont’d) •Induction of a fibrinolytic state by the infusion of plasminogen activators is therapy for some thromboembolic disorders. •Fibrinolytic therapy is used in patients with massive pulmonary embolism and to restore the patency of acutely occluded arteries. •Prompt fibrinolytic therapy can reduce both myocardial damage and mortality following acute coronary occlusion.