Download
1 / 18
250 likes | 716 Views
Hypersensitivity Reactions (HSRs). Objectives. The learner will be able to: Know the signs and symptoms hypersensitivity reactions (HSRs). Verbalize the proper emergency management of a suspected HSR. Problem and Incidence. Cancer therapies have the potential to cause HSRs.

E N D
Objectives The learner will be able to: • Know the signs and symptoms hypersensitivity reactions (HSRs). • Verbalize the proper emergency management of a suspected HSR.
Problem and Incidence • Cancer therapies have the potential to cause HSRs. • These reactions may be triggered by the therapeutic agent, the diluent, or the solution. • The general incidence of HSRs is 5%, but the incidence for some agents is much higher.
Hypersensitivity Reactions • Reactions are either anaphylactic or anaphylactoid. • Anaphylactic reactions to chemotherapy agents are allergic reactions mediated by the release of Ig-E from the immune system. • Anaphylactoid reactions are not mediated by Ig-E and caused by the release of cytokines.
Hypersensitivity Reactions • There are various types of HSRs; some are localized and mild, others are generalized and moderate to severe, and still others are life-threatening.
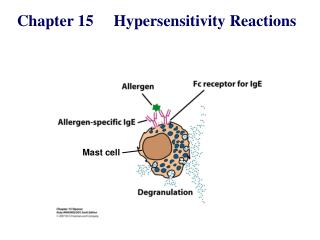
Immune System Function in Anaphylactic Reactions • An antigen is recognized as foreign. • The body forms antibodies as part of an adaptive immune response. • The most common antibody or immunoglobulin formed during an allergic reaction is Ig-E. • Ig-E promotes histamine release from mast cells and basophils.
Hypersensitivity and Anaphylaxis • HSRs are more likely to occur with the second dose of an agent but can occur with the first. • Symptoms can range from itching at the injection site to systemic shock. • The response usually occurs within 5-10 minutes of the initiation of therapy. Quicker onset of symptoms increases the severity of the reaction. • Delayed reactions can occur 10-12 hours after administration.
Immune System Function in Anaphylactoid Reactions • Immune response to a foreign antigen (drug or substance) causes T lymphocytes actions to result in the release cytokines.
Immune System Function in Anaphylactoid Reactions • Cytokines are proteins that help coordinate immune and inflammatory responses. • Cytokines that mediate inflammatory responses include interleukines, interferons, and tumor necrosis factors. • Cytokine release can cause fever, chills, headache, nausea, fatigue, and hypertension.
Hypersensitivity Reactions • Although anaphylactic and anaphylactoid reactions differ in their origin, the clinical symptoms can be the same for both reactions. • Therefore, the management is the same for both types.
Risk Factors for All Hypersensitivity Reactions • Chemotherapy and biotherapy are known to cause hypersensitivity. • High doses of high risk agents • IV administration of high risk agents • Agents derived from bacteria and L-asparaginase • Crude preparations of agents, such as phase 1 studies
Risk Factors for All Hypersensitivity Reactions • Preexisting allergies, especially to food, drugs, bee stings, blood products, and contrast dye • Previous exposure to the agent • Carboplatin reaction risk increases at the sixth infusion and peaks at the eighth infusion • Oxalipatin reactions occur more frequently after five cycles • Failure to administer pre-meds
Preadministration Guideline • Obtain and record baseline vital signs. • Review allergy history. • Administer pre-medications. • Antipyretic • Histamine blocker (H1 and H2) • Corticosteroid • Ensure emergency meds are available, and preferable to have an order to use prior to treatment. • Instruct patient on signs and symptoms to report. • Perform scratch test or intradermal skin test if recommended.
Clinical Manifestations • Uneasiness or agitation • Tightness in the chest • Shortness of breath with or without wheezing • Hypotension • Tachycardia • Headache • Urticaria or rash • Localized or generalized itching • Periorbital or facial edema • Lightheadedness or dizziness • Abdominal cramping, diarrhea, nausea, or vomiting
Emergency Management • Stop infusion • Maintain an IV line with saline • Stay with patient; call for help • Place patient in supine position—legs elevated if hypotensive • Monitor vital signs • Maintain an airway • Administer or order emergency medications • Diphenhydramine, Famotidine, Corticosteroids, Epinephrine • Provide emotional support • Document treatment and responses • Remember that symptoms may reoccur
Managing Reactions Caused by Cytokine Release • Most of these reactions are caused by monoclonal antibodies. • Unlike anaphylaxis, cytokine release reactions often can be managed by short-term cessation of the infusion and administration of histamine blockers, and restarting the infusion at a slower rate.
Patient and Family Teaching • Prior to administration of agents, teach patients that HSRs are a possibility. • Instruct patients about what symptoms to report. • After therapy, talk to patients about risk for delayed or recurrent reaction.
References Povolich, M., Whitford, J.M., & Olsen, M. (Eds.). (2009). Chemotherapy and biotherapy guidelines and recommendations for practice. Pittsburgh, PA: Oncology Nursing Society. Viale, P.H. (2010). Dermatologic complications. In J. Eggert (Ed.), Cancer basics (pp. 378-377). Oncology Nursing Society: Pittsburgh, PA. Viale, P.H., & Sanchez-Yamamoto, D. (2010). Biphasic and delayed hypersensitivity reactions: Implications for oncology nursing. Clinical Journal of Oncology Nursing, 14(3), 347-356. Vogel, W.H. (20120). Infusion reactions: Diagnosis, assessment, and management. Clinical Journal of Oncology Nursing, 14(2), E10-E21.