Download
1 / 35
420 likes | 1.32k Views
HYPERSENSITIVITY REACTIONS. II BPT Dr Ekta Chourasia Department of Microbiology. What is hypersensitivity?. Injurious consequences in the sensitized host, following contact with specific antigen

E N D
HYPERSENSITIVITYREACTIONS II BPT Dr Ekta Chourasia Department of Microbiology
What is hypersensitivity? • Injurious consequences in the sensitized host, following contact with specific antigen • Deals with injurious aspect of heightened andexaggerated immune response leading to tissue damage, disease or even death • Concerned with what happens to the host rather than what happens to the antigen. Dr Ekta, Microbiology
Musts for Hypersensitivity • Contact with allergen • Sensitizing/priming dose • Induction of AMI/CMI • Shocking dose Dr Ekta, Microbiology
Classification • Based on the time required for a sensitised host to develop reactions on re-exposure to the Ag • Immediate hypersensitivity (B cell or Ab mediated) – Anaphylaxis - Atopy - Ab mediated cell damage - Arthus phenomenon - Serum sickness • Delayed hypersensitivity - Tuberculin type - Contact dermatitis Dr Ekta, Microbiology
Immediate Appears & recedes rapidly. Induced by Ags or haptens by any route. ‘Ab mediated’ reaction. Delayed Appears slowly, lasts longer. Ag or hapten (ID) or with Freunds adjuvant or by skin contact. ‘Cell mediated’ reaction. Immediate Vs Delayed Hypersensitivty Dr Ekta, Microbiology
Classification • Based on the Mechanism ofPathogenesis – Coombs & Gell (1963) classification (4 types) • Type l : IgE mediated • Type ll : Cytolytic & Cytotoxic • Type lll : Immune complex • Type lV : Delayed hypersensitivity Dr Ekta, Microbiology
Coombs & Gell Classification (1963) Dr Ekta, Microbiology
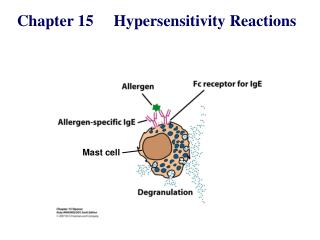
Type I reactions • IgE dependent. • Occur in 2 forms: • Anaphylaxis – acute, potentially fatal, systemic form. • Atopy– chronic or recurrent, non fatal, localized form. Dr Ekta, Microbiology
Anaphylaxis • Classical immediate hypersensitivity reaction • Sensitization • Most effective when Ag is introduced parenterally • Minute quantities are enough • Interval of 2-3 wks needed between sensitizing & shocking dose • Once sensitized it remains so for long time • Shocking dose most effective by IV route then IP, then SC then ID • The shocking Ag must be same or similar to Sensitizing Ag Dr Ekta, Microbiology
B cell IL13 TH2 Newly synthesized mediators Sensitization against allergens and type-I hypersensitivity Histamine, tryptase, kininegenase, ECFA Leukotriene-B4, C4, D4, prostaglandin D, PAF
Type I Reactions • Humans – • Itching of scalp & tongue, flushing of skin, difficulty in breathing, nausea, vomiting, diarrhea, acute hypotension, loss of consciousness, death (rare) • Causes • Serum therapy, antibiotics, insect stings • Treatment • Adrenalin 0.5 ml (1 in 1000 solution) SC/IM repeated up to 2 ml in 15 min Dr Ekta, Microbiology
Cutaneous (Local) Anaphylaxis • Follows I.D. injection (small shocking dose) – a local wheal &flare response is seen. • Wheal – central pale area of puffiness due to edema • Flare - surrounds wheal, caused by hyperemia and subsequent erythema. Uses : - Testing for hypersensitivity • Precaution – Keep adrenalin injection ready to combat severe fatal reaction. Dr Ekta, Microbiology
Atopy • Refers to naturally occurring familial hypersensitivities of human beings : - Hay fever - Asthma • Ags involved in atopy can be • Inhalants – pollen, house dust • Ingestants – eggs, milk • Contact allergens. Dr Ekta, Microbiology
Type-I hypersensitivity The common allergy Dr Ekta, Microbiology
Diagnosis • Skin tests (ID injection ) - with allergens like pollen, cat or dust mite Children - 3x3 mm wheal Adults – 4x4 mm wheal +ve test takes 5 -15 mins to develop, persist for 30 mins or more – IMMEDIATE RESPONSE. 2. Radioallergosorbent test (RAST) - to measure the levels of Ig E in serum. Dr Ekta, Microbiology
Type II (Cytotoxic) Reactions • Involve activation of complement by IgG or IgM binding to an antigenic cell. • Antigenic cell is lysed. Dr Ekta, Microbiology
Type II Hypersensitivity Role of complement and phagocytes Dr Ekta, Microbiology
Examples of Type II Hypersensitivity Reactions • Reactions against blood cells & platelets • Incompatible blood transfusion. • Hemolytic disease of the newborn. • Autoimmune hemolytic anemias, thrombocytopenia. • Reactions against Tissue Antigens • Myasthenia gravis • Pemphigus vulgaris Dr Ekta, Microbiology
Type II hypersensitivity induced by exogenous agents Dr Ekta, Microbiology
Type III (Immune Complex) Reactions • Involve reactions against solubleantigens circulating in serum. • Usually involve IgA antibodies. • Antibody-Antigen immune complexes are deposited in organs, activate complement, and cause inflammatory damage. • Glomerulonephritis: Inflammatory kidney damage. • Occurs when slightly high antigen-antibody ratio is present. Dr Ekta, Microbiology
APC B cell TH2 Sensitization for Type III hypersensitivity Dr Ekta, Microbiology
Immune Complex Mediated Hypersensitivity Dr Ekta, Microbiology
Serum Sickness • Systemic form of type lll HS. • Appears 7-12 days following the injection of large doses of foreign serum. • ICs are deposited on the endothelial lining of blood vessels in various parts of the body. • Features – fever, LN pathy, splenomegaly, arhthritis, glomerulonephritis, endocarditis, rashes, abdominal pain, nausea & vomiting. Dr Ekta, Microbiology
Serum sickness Dr Ekta, Microbiology
Arthus Reaction • Local reaction consisting of edema, induration & hemorrhage. • Follows SC injection with a foreign serum. • Reaches peak after 4 - 10 hrs, disappears by 48 hrs. Dr Ekta, Microbiology
Type 4: Delayed Hypersensitivity • Takes more than 12 hrs to develop. • Involve CMI reactions. • Provoked by intracellular microbialinfections or haptens like simple chemicals • Varieties of Delayed HS : • Contact 48-72 hrs • Tuberculin 48-72 hrs • Granulomatous 21-28 days Dr Ekta, Microbiology
Contact Dermatitis • Eczematous reaction at the point of contact with an allergen, like • Metals – nickel, chromium • Simple chemicals – dyes • Drugs – Penicillin • Cells involved in Contact HS • Langerhans cells • Keratinocytes Dr Ekta, Microbiology
Contact Dermatitis • Lesions – vary from macules & papules to vesicles that break down leaving behind raw weeping areas • Detected by ‘Skin Patch Test’ * Allergen is applied to the skin under an adherent dressing. * Itching appears in 4- 5 hrs. * Local reaction after 24- 48 hrs: Erythema to vesicle or blister formation Dr Ekta, Microbiology
Clinical & Patch test appearance of contact hypersensitivity Dr Ekta, Microbiology
Tuberculin Type Hypersensitivity • Tuberculin type – • ID inoculation of PPD in sensitized individual leads to induration & inflammation in 48-72 hrs. This is not the same as skin test done for Type I hypersensitivity. • Used for diagnosis / exclusion of diagnosis of many bacterial / fungal / parasitic / viral and autoimmune diseases. Dr Ekta, Microbiology
Diseases Manifesting Granulomatous HS • Leprosy • Tuberculosis • Schistosomiasis • Sarcoidosis • Crohn’s disease Dr Ekta, Microbiology
characteristic Type-I Type-II Type-III Type-IV antibody IgE IgG, IgM IgG, IgM none exogenous cell surface soluble intracellular antigen response time 15-30 min. Min.-hrs 3-8 hours 48-72 hours or longer Erythema & edema Erythema & induration Lysis & necrosis appearance Weal & flare baso- and eosinophils Ab and complement Monocytes & lymphocytes histology PMN and complement antibody T-cells antibody transfer with antibody examples hay fever, asthma pemphigus, Goodpasture farmers’ lung, SLE TB test, poison ivy, granuloma Comparison of hypersensitivity reactions Dr Ekta, Microbiology