Download
1 / 25
250 likes | 583 Views
Hypersensitivity Reactions. Dr. Raid Jastania. Hypersensitivity Reactions. Normal immune reactions Can be harmful Examples of these diseases: bronchial asthma, allergic reactions, immune-mediated hemolysis, immune-mediated arthritis, transplant rejection. Antigen.

E N D
Hypersensitivity Reactions Dr. Raid Jastania
Hypersensitivity Reactions • Normal immune reactions • Can be harmful • Examples of these diseases: bronchial asthma, allergic reactions, immune-mediated hemolysis, immune-mediated arthritis, transplant rejection.
Antigen • antigen is any molecule (proteins or others) that trigger the immune response and activates humoral or cellular immunity. • exogenous like bacteria, viruses, fungi, parasites, or allergen • indogenous from the cells or the extracellular matrix, like DNA, nuclear molecules, surface receptors, or desmosomes. • intracellular or extracellular. • single exposure or continuous over long period.
Immune system • When the immune system is activated against an antigen, there is activation of either cellular immunity or humoral immunity. • Why some antigens trigger cellular immunity and others trigger humoral immunity is not well understood. • extracellular antigens (bacteria) activate the humoral immunity • intracellular antigens (viruses) activate the cellular immunity.
Immune System • Ag-Ab complex • normally removed by phagocytic cells • if it persists it may activate the complement system and initiates inflammation. • IgG and IgM are the complement-fixing • IgA can activate the alternative complement pathway. • IgE mediates the response to parasites and mediate allergic responses.
Immune System • Cellular immunity: • CD4+ T-cell • CD8+ T-cell
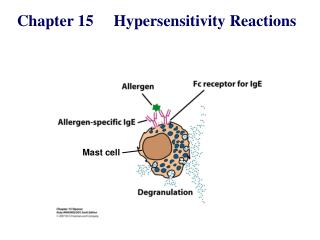
Type I Hypersensitivity (Allergy and Anaphylaxis) • Events: • Exposure to antigen (allergen) • Antigen is processed and presented by APC on MHC-II • Stimulate T-cell response, Th2 (IL4, IL5) • Induce B-cell to mature and produce IgE • IgE is bound to Fc receptor on mast cells and basophils • Those mast cells are armed by IgE and ready to react
When re-exposure to antigen (allergen) occurs it binds to IgE and activates the mast cells and degranulation • This result in release of primary and secondary mediators • Primary mediators including: • Histamine causing vasodilatation, bronchospasm and increase mucus secretion • Adenosine causing bronchospasm • Heparin
Secondary mediators including: • Arachidonic acid (AA) metabolites: leukotrienes and prostaglandins (PG) • LTC4, LTD4 very potent spasmogenic, and chemotactic agents attracting eosinophils and monocytes • PGD2 resulting in bronchospasm and increase mucus secretion • Cytokines: TNF, IL-1, IL-4, IL-5, IL-6.
Mast cells • Found near blood vessels, nerves, and in subepithelial region • Contain secretory granules • IgE bound to surface and activate them • Can be activated by drugs (codeine, morphine), physical heat and cold and sunlight
Localized type • Examples: hay fever, allergic rhinitis, bronchial asthma, food allergy • Familial suseptability • Exposure by skin contact, inhalation or ingestion. • 2 phases: • Initial phase: (5-30 minutes) mast cell degranulation and release of primary mediators resulting in vasodilatation, vascular leakage, smooth muscle spasm. • Late phase reaction: (2-8 hours) and last for days. It is mediated by secondary mediators and recruitment of eosinophils and other inflammatory cells
Systemic Anaphylaxis • Pareneral administration of allergen, eg. Drugs like penicillin • Urticaria, skin erythema occurs in minutes of exposure • Pulmonary bronchospasm and increase secretion of mucus • Laryngeal edema, Vomiting and diarrhea • Vasodilatation (anaphylactic shock)
Type II Hypersensitivity • Events: • Antigen is present of the surface of cells or extracellular in tissues • Can be intrinsic or extrinsic antigen • Antibody binds to antigen and followed by one of the following: • Complement-dependent reaction • Resulting in direct lysis of cells by MAC • Or by opsonization and phagocytosis by macrophages
Type II Hypersensitivity • Events: 2. Antibody-dependent Cell-mediated cytotoxicity (ADCC): • Target cells are coated with Ab (commonly IgG) • Cells are lysed by neutrophils, eosinophils, macrophages, or NK cells. 3. Antibody-mediated cellular dysfunction Example: Myasthenia gravis, Graves disease of thyroid
Type II Hypersensitivity • Examples: • Transfusion reactions (incompatible RBC from donor) • Erythroblastosis fetalis: incompatible Rh antigen • Autoimmune hemolysis and autoimmune thrombocytopenia • Drug reactions to penicillin • Pemphigus vulgaris: antibody to desmosome • Good pasture syndrome
Type III Hypersensitivity (Immune Complex Disease) • Events: • There are 3 phases: • Ag-Ab complex formation • Deposition of Ag-Ab complex • Injury by acute inflammation
Acute Serum Sickness: • It is a typical example of immune complex disease. It occurs when horse anitetanus serum is administered, or when horse antithymocyte globulin is administered for the treatment of apalstic anemia. • After 5 days, Ab is formed and Ag-Ab complex is formed • Ag-Ab complexes are deposited in tissue. Deposition is dependent on several factors
Acute Serum Sickness: • Deposition of complexes depends on: • Size of complexes • Status of mononuclear phagocytic system • charge of complexes, affinity of Ag to tissues, and the structure of the complexes and the hemodynamics at the site of deposition. • Favored site of deposition are: Kidneys, joints, skin, heart, serosal surfaces and small blood vessels in any tissue.
Acute Serum Sickness: • After deposition (10 days) there is activation of the complement system and acute inflammation resulting in tissue injury. • Immune complexes activates Hageman factor, as well, and result in thrombosis.
Examples: • The reaction can be localized or systemic • Exposure to Ag can be single event or continuous chronic diseasea. • Acute serum sickness is systemic. • SLE is typical example of immune complex disease. • Arthus reaction • Glomerulonephritis, Arthritis, carditis, Serositis, vasculitis.
Type IV Hypersensitivity • It is cell-mediated reaction occurring in response to: • intracellular organisms (virus, TB) • Extracellular fugi or parasite. • It includes 2 types of sensitized T-cells: • CD4+ T helper cells mediate delayed-type hypersensitivity • CD8+ cytotoxic T-cell mediate Cell-mediated cytotoxicity
Delayed-type Hypersensitivity • Events: • Ag processed and presented by APC to CD4+ Th1 cells (IL-2, IFN-gamma) • T-cell is sensitized and stay as memory cells. • When re-exposure to Ag occurs, sensitized T-cell is activated, proliferate and secrete mediators • The result is erythema and induration, Activation of macrophages. • IL-12, IFN-gamma, IL-2, TNF
Delayed-type Hypersensitivity • Examples: • Tuberculin skin test in a sensitized person • Contact dermatitis • Granulomatous inflammation is a special type of delayed hypersensitivity. • It results from non-degradable antigen with T-cell reaction. After 2-3 weeks there is aggregates of macrophages that become epithelioid and form giant cells.
T-Cell Mediated Cytotoxicity • Mediated by sensitized CD8+ cytotoxic cells • The aim is killing of cells bearing the Ag by: • Perforin-granzyme • Fas-Fas ligand killing
T-Cell Mediated Cytotoxicity • Examples: • Graft rejection • Tumor immunity