Download
1 / 37
370 likes | 381 Views
A Practical Approach to The Diagnosis and Evaluation of Headache & Seizures. Dr. Fawad Ahmad Randhawa M.B.B.S. ( King Edward Medical College) M.C.P.S; F.C.P.S. ( Medicine) F.C.P.S. ( Endocrinology) Assistant Professor of Endocrinology King Edward Medical University. Objectives.

E N D
A Practical Approach to The Diagnosis and Evaluation of Headache & Seizures Dr. Fawad Ahmad Randhawa M.B.B.S. ( King Edward Medical College) M.C.P.S; F.C.P.S. ( Medicine) F.C.P.S. ( Endocrinology) Assistant Professor of Endocrinology King Edward Medical University
Objectives By the end of first session, students should be able to Importance of headache Comprehend the basis of seizures
Learning Outcomes • Know what causes headache • Most common and important causes of headache • Remember warning signs of headache
Painful structures Skin, Subcutaneous tissue, Muscles, Bones, Periosteum of the skull (Injury, swelling, infection, tumor, etc.) Meninges, (Meningitis) Arteries within the meningeal spaces (Migraine, Vasculitis) Teeth Eye, Ear, Nasal cavity and sinuses (Must ask)
Painful structures • Cranial nerves 5 (Trigeminal nerve) • Face and anterior half of skull, Meninges, Vessels around the meninges • Cranial nerve 7 (Facial nerve) • Cranial nerve 9, and 10 • Cervical nerves 1, 2, and 3 • Receive pain from occipital area, basal meninges
To summarize…… Disorders of cranial bones Disorders of eyes Disorders of ears Rhinosinusitis Disorders of teeth and jaws, TM joints Disorders of neck
Muscles causing headache Tension headache
Vessels causing headache • Migraine • Cluster headache • Vasculitis/Arteritis (Temporal arteritis/Giant cell arteritis) • Vascular bleed • Intracranial • Subarachnoid
Dangerous symptoms in Headache • Sudden or progressive headache • Pressure symptoms, e.g. vomiting, increased pain with coughing or straining, worse just after awakening • Systemic symptoms (e.g., fever, weight loss) • Focal Neurologic symptoms or signs (seizures, paresis or sensory loss in some part of body) • Secondary risk factors (e.g., cancer, HIV)
Learning outcomes By the end of second session, students should be able to • Define seizure • Define epilepsy • Classify seizures • Comprehend the basic investigation tools for the diagnosis of seizure disorders
Three basic questions • Is it a seizure? If so, what kind? • What caused it? • What should be done?
Seizure A seizure is a set of clinical symptoms associated with abnormal electrical activity in neurons in the cortex of the brain. The clinical characteristics of a seizure are the result of the area of the brain that is abnormally stimulated.
Epilepsy Clinical condition in which there are multiple seizures that are unprovoked.
Seizures - Classification • Focal seizures – account for 80% of adult epilepsies • Generalized seizures • Unclassified seizures
Seizures Partial • Electrical discharges in a relatively small group of dysfunctional neurones in one cerebral hemisphere • Aura may reflect site of origin • + / - LOC Generalized • Diffuse abnormal electrical discharges from both hemisphere • Symmetrically involved • No warning • Always LOC
Partial Seizures Simple Secondary generalized Complex 1. w/ motor signs 2. w/ somato-sensory symptoms 3. w/ autonomic symptoms 4. w/ psychic symptoms 1. simple partial --> loss of consciousness 2. w/ loss of consciousness at onset 1. simple partial --> generalized 2. complex partial --> generalized 3. simple partial --> complex partial --> generalized
Generalized seizures- types • Primary generalized seizures (grand mal) • Absence seizures (petit mal) • Myoclonic seizures • Atonic seizures • Tonic
Aetiology of seizures Epileptic • Idiopathic (70-80%) • Cerebral tumour • Neurodegenerative disorders • Secondary to • Cerebral damage: e.g. congenital infections, intraventricular haemorrhage • Cerebral dysgenesis/malformation: e.g. hydrocephalus
Aetiology of seizures Non-epileptic • Febrile convulsions • Metabolic • Hypoglycaemia • HypoCa, HypoMg, HyperNa, HypoNa • Head trauma • Meningitis • Encephalitis • Poisons/toxins
Diagnosis is largely based on the history of the event • Precipitating factors • Position, activity, intercurrent illness, medications • Description of the episode • Eye movements, body movements, one sided or both sides, loss of consciousness or alteration of consciousness, incontinence, duration, aftereffects • Predisposing factors • Past medical history, recent illness or neurological symptoms, family history • Is it a seizure, if so what kind?
Idiopathic seizures • The cause of the seizure can not be determined by conventional testing or • Seizures of genetic origin in which seizures are the only manifestation. • This category may comprise as much as 60% of all childhood seizure disorders.
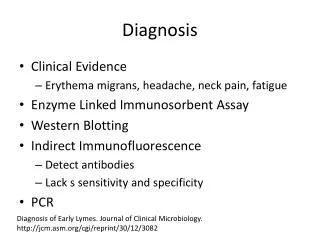
Investigations I. Exclusion of differentials: • Bedside: urinalysis • Hematological: CBP • Biochemical: U&Es, Calcium, glucose, ABGs • Radiological: CXR, CT head • Toxicological: screen • Microbiological: LP (Always used with justification)
Investigations II. Confirmation of epilepsy: • Dynamic investigations : result changes with attacks • E.g. EEG • Static investigations : result same between and during attacks • E.g. Brain scan
Electroencephalography (EEG) • EEG indicated whenever epilepsy suspected • Uses of EEG in epilepsy • Diagnostic: support diagnosis, classify seizure, localize focus, quantify • Prognostic: adjust anti-epileptic treatment
Neuroimaging • Structural neuroimaging • Functional neuroimaging
Structural Neuroimaging Modalities available: • Magnetic Resonance Imaging (MRI) • Computerized Tomography (CT) What sort of structural scan? • MRI better than CT • CT usually adequate if to exclude large tumor • MRI not involve ionizing radiation
Functional Neuroimaging • Principles in diagnosis of epilepsy: • When a region of brain generates seizure, its regional blood flow, metabolic rate and glucose utilization increase • After seizure, there is a decline to below the level of other brain regions throughout the interictal period
Treatment Decisions The decision to treat depends on evaluation of risks and benefits • Risk of subsequent seizures • Risk of treatment • Particular circumstances of patient • What to do about it?
Risks of further seizures • Risk of a second seizure is 20-30% if: • Examination, EEG and CT (imaging study) is normal (and careful review of history discloses no other events) • Risk of a second seizure if EEG is abnormal is 60%
Risk of having another seizure • Most seizures do not produce injury to the brain. • Seizures in a bad place- bath, driving a car, climbing, riding a bicycle etc. • Prolonged seizure which can lead to hypoxia or secondary complications. • Sudden unexplained death- a very rare complication of seizures, particularly in children.
Risk of treatment Medication side effects • Severe- liver failure, aplastic anemia, severe allergic reaction (Stevens-Johnson syndrome) • Decreased alertness, personality/behavior changes, weight loss/gain Social stigma
Treatment • Discuss risks and benefits with patient and parent based on available statistics • If 1st seizure with lower risk of recurrence, consider no treatment. • Use of rectal valium as a “rescue measure” • If decision to treat, choose a medication based on seizure type, age of patient and side effect profile. • Monotherapy is generally preferable, especially in first line treatment.
Anticonvulsant medications Generalized seizures • Divalproex sodium • Zonisamide • Topiramate • Lamotrigine • Levetiracetam • Rufinamide • Ethosuximide Partial Seizures • Carbamazepine • Oxcarbazepine • Zonisamide • Topiramate • Levetiracetam • Lamotrigine • Phenytoin • Phenobarbital
Generalized seizures vs Partial Seizures- Recap • Generalized seizures have sudden onset without warning. Motor symptoms are symmetrical. Postictal state is common when there is convulsive activity but not for absence or myoclonic seizures • Partial seizures may begin with localized symptoms that the patient is aware of (aura) and may have asymmetric motor symptoms. Postictal state is common, even without convulsive activity