Download
1 / 22
240 likes | 377 Views
PSORIASIS. Kate Blake Lead Nurse Dermatology. Psoriasis. Is a chronic inflammatory skin disease Affects 3% of U.K. population 75% are successfully managed in the community with topical treatments (Griffiths,2004) Also common in India, Far East and parts of Africa. Cause.

E N D
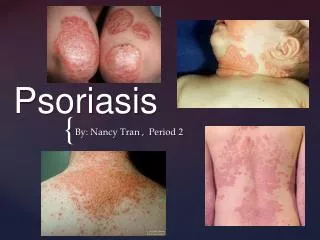
PSORIASIS Kate Blake Lead Nurse Dermatology
Psoriasis • Is a chronic inflammatory skin disease • Affects 3% of U.K. population • 75% are successfully managed in the community with topical treatments (Griffiths,2004) • Also common in India, Far East and parts of Africa
Cause • Strong genetic link • No clear cut inheritance pattern • Poorly understood
Infection Medication Alcohol & Smoking Climate Change Skin Trauma Stress Trigger Factors
Pathology • Epidermal Hyperproliferation • Accumulation of inflammatory cells • Increased vascularity of the upper dermis
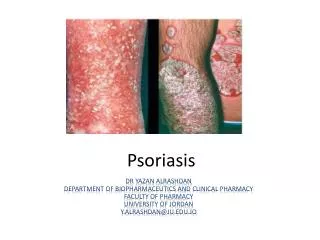
Chronic Plaque Psoriasis • Most common • Single or multiple plaques • Red, scaly surface • Vigorous rubbing causes capillary haemorrhage
Chronic Plaque Psoriasis • Predilection for knees, elbows, base of spine • Symmetrical, chronic, & stable • mms to cms in diameter • Sometimes causes itching
Treatment Options • Dithranol / Micanol • Dovonex / Dovobet • Topical steroids • Coal Tar • Ultra Violet Light • Systemics • Biologics
Guttate Psoriasis • Often follows sore throats • Common in young adults • Lesions about 1 cm diameter • Paler pink than established psoriasis • Often resolves rapidly • May enlarge & become stable plaques
Treatment Options • Tar based ointment • Dovonex ; Dovobet • Ultra violet light • Ultra violet light plus tar based ointment • Ultra violet light plus Dovonex
Flexural Psoriasis • May accompany plaque psoriasis • Occurs in groin,natal cleft, axillae & submammary folds • Maceration leaves beefy erythematous rash • Often itchy • Subject to secondary contact sensitivity
Treatment Options • Can be problematic • Mild tar/corticosteroid mixtures may be effective • Steroids can cause striae • Low concentrations of dithranol may burn delicate areas • nUVB & PUVA can be effective if area is accessible
Scalp Psoriasis • Common • Scalp alone may be affected • Lesions very small to whole scalp cover • Occasionally thick and sticks in large chunks to hair • Temporary hair loss
Treatment Options • Tar shampoos • Betamoose • Scalp Blitz • UV combs
Chronic Palmo-plantar Psoriasis • Usually found alone • Erythematous with numerous pustules • Pustules become brown scaly spots & peel off • Painful • Small area or entire surface of palms or soles • May cause considerable disability
Treatment Options • Topical treatments often ineffective • PUVA may give some control • Relapse is common
Nail Psoriasis • Nail involvement frequent • Nail pits • Onycholysis • Can become discolored • Painful • Whole surface may become damaged
Exfoliative Erythroderma • Dermatological emergency • Plaques merge to cover most of skin • Can be slow or rapid • Systemic/ topical steroids may precipitate
Acute Pustular Psoriasis • Dermatological emergency • With or without pre existing psoriasis • Sudden development of widespread erythema • Pustules are sterile • May coalesce to form lakes of pus • High swinging temperature and unwell • Patient may die from secondary infection
Psoriatic Arthropathy • Affects up to 10% of people with psoriasis • Is erosive and may result in joint destruction