Download

1 / 28
280 likes | 539 Views
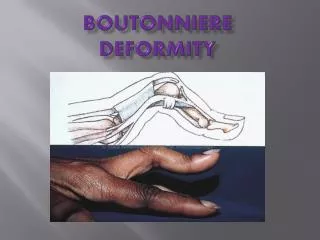
Correction of varus deformity. Varus deformity: is the most common deformity of the ostearthritis knee, and multiple techniques have been described for its correction.

E N D
Correction of varus deformity • Varus deformity: is the most common deformity of the ostearthritis knee, and multiple techniques have been described for its correction. • The surgeon should understand which anatomic structure will affect the extension and flexion gaps so that each individual type of gap asymmetry can be properly corrected.
Correction of varus deformity • The first remove all osteophytes on the femur and the tibia because thay can tent medial soft tissue sleeve and effectively shorten the MCL. • Make the initial exposure to include release of the deep MCL off the tibia to the posteromedial corner of the knee.
Correction of varus deformity • If the extension gap is tight only medially, release the posterior oblique ligament and semimembranous on the tibia. • If the flexion gap is tight, release the anterior half of the superficial MCL and the Pes anserinous • If the entire soft tissue sleeve is released and the medial gap is still tight (in severe varus) consider advancing the L.C.L
Correction of varus deformity • PCL: make sure the PCL is resected before balancing. • Because the PCL is a secondary medial stabilizer, take care not to release the entire soft tissue sleeve off the tibia because it may overshoot the gap. • Is general, less soft tissue release is needed to balanced a varus knee once the PCL is resected.
Correction of varus deformity Assess the flexion and extension gaps • If the gaps are tight: Release the superficial MCL incompletely on tibia. • If the extension gap is tight: Release P.O.L and semimembranous. • If the flexion gap is tight: Release the superficial MCL completely and Pes.
Correction of varus deformity • Bony deformity: when deformity is fixed and nonreducible, and in late stage, some degree of bone erosion is often present at the concave side of the deformity, where ligament and knee capsule are contracted. • Significant varus or valgus malaligament on the coronal plane is very often associated with sagital plan and torsional deformities.
Correction of varus deformity • Two points: That we must attention. • With significant flexion deformity, the surgeon may need more extensile soft tissue work on the posterior capsule and gasterocnemius insertion. • Extraarticular diaphyseal or metaphyseal deformity are often associated with fixed deformity at the joint line and possibility need to correcting the deformity at the joint level with generous bone resection and ligament release or a combined osteotomy.
Correction of varus deformity • Pagoda: in advanced deformity, the tibial medial platateau develops a concave pagoda shape in which the femoral condyle is embedded, leading to a difficult tibial dislocation maneuver that may harm the MCL. • In these cases, we suggest violating the posterior tibial osteophyte with a straight osteotome between tibia and femur at 90 degree of flexion. • In severe cases we prefer to remove the PCL and to use a PCL substituting.
Correction of varus deformity • After a bone cuts and primary release, if some medial residual tension remains, the distal insertion of superficial of MCL is released at least & to 10cm from the joint line. • Alternatively, the MCL could be pie-crusted with a 16-gauge needle with multiple punctures. • In advanced fixed varus we must select a small tibial size to lateralized it. • This causes remove the exposed medial sclerotic bone, which is tenting the medial structures both in extension and in flexion.
Correction of valgus deformity • Valgus deformity is common in Rheumatoid and inflammatory arthritis and in patients with hypoplastic lateral femoral condyle or previous trauma or osteotomies. • The three layer anatomy of the lateral side of the knee joint makes its soft tissue balancing more complex than with varus deformity.
Correction of valgus deformity • During exposure of a knee with valgus deformity, take care not to compromise the medial soft tissue sleeve. • The first release of the lateral side and release the lateral capsule from tibia. • The second stage depends on whether both the extension and flexion gaps are right. If both are tight, release the LCL off the lateral epicondyle, taking care to leave the insertion of the popliteus intact.
Correction of valgus deformity • If only the extension gap is tight: release the iliotibial band by a Z lengthening or pie-crusting of the band two cm above Joint line. • Release of the posteromedial corner has been shown to effectively increase the extension space more than the flexion space. • Release of the popliteus tendon will increase the flexion gap laterally more than the extension.
Correction of valgus deformity • If the knee is still not balanced in full extension after release of all three structures, release the posterior capsule off the lateral femoral condyle. Then release the lateral Head of gasterocnemious, if further correction is needed. • PCL is a medial structure and often is lengthening in a valgus knee but sometimes is involved in the deformity.
Correction of valgus deformity • If complete release of all of above structures, dose not balanced the flexion and extension gaps, consider advancement of the MCL. • If the lateral flexion gap opens more than the flexion gap, make certain, that the ”Jump height” of a posterior stabilizing peg is not exceeded and consider using CCK.
Correction of valgus deformity • Pie-crusting technique: Is another technique used for soft tissue balancing in valgus knee, and allows direct lengthening of taut soft tissue under tension of the joint space. • Multiple stabs wound are made with a scalpel blade parallel to joint line. • There are multiple studies with good results for both valgus and varus. • The advantage is that it leaves supporting tether and not allow a large gap opening on the lateral side of knee in extension.
Correction of valgus deformity • Bone deformity: Intraarticular bone deformity can be recognized preoperatively. • Hypoplasia:of lateral femoral condyle in valgus knee and possible need for augmentation and ipertrophic medial femoral condyle in varus knees and to achieve a stable and rectangular flexion gap must be attention.
Correction of valgus deformity • Approach: we believe it is possible to safety address all valgus deofromities from a medial Parapatellar approach, but some surgeons advocate the need for a lateral approach for a directly to pathology • For some severe cases there is need to tubercle osteotomy. • In these cases there is lateral capsular closure difficulties and need to use fat pad.
Correction of valgus deformity • For severe cases, we suggest some degree of overcorrection for distal cut and must select 4 degree and attention is paid to select entry point more medial than usual. • Tibial resection is performed perpendicular to the mechanical axis as usual. • AP Femoral bone resection are performed using all available landmarks with a special focus on the epicondyles.
Correction of valgus deformity • In vaglus knees because of lateral condyle hypoplasia, requiring additional degrees of external rotation related to the posterior condyle axis. • Valgus knees usually are more deformed in extension than in flexion. • This makes the posterior capsule and the iliotibial band the most frequently contracted structures.
Correction of valgus deformity • The LCL is also contracted in more than 50% of cases and the popliteal tendon is less involved. • Our preferred lateral release techniques is pie-crusting techniques performed with multiple punctures with the knee in extension and the laminar spreader distracting the knee joint space, the contracted structures are palapted, A no 15 small blade is used to perform a capsular incision at the level of the tibial bone cut off the posterior capsule.
Correction of valgus deformity • In severe valgus deformity recommended: • Use a lateral approach an pie – crusting technique for balancing. • Use a constrain condylar knee • Use Hofaplasty technique for closure of joint