Download
1 / 31
310 likes | 547 Views
introduction to the design of diagnostic criteria. Joop P van de Merwe Dept. of Immunology & Internal Medicine Erasmus MC Rotterdam j.vandemerwe@erasmusmc.nl ESSIC Meeting Baden 16-18 June 2005. * Fries JF et al . Arthritis Rheum 1994;37:454-62. All Persons. Persons with Diseases.

E N D
introduction to the design of diagnostic criteria Joop P van de MerweDept. of Immunology & Internal MedicineErasmus MC Rotterdamj.vandemerwe@erasmusmc.nlESSIC Meeting Baden 16-18 June 2005
All Persons Persons with Diseases Persons with Confusable Diseases Persons with Target Disease CLASSIFICATION CRITERIA* Classification criteria separate patients with the disease from the general population and from patients with potentially confusable conditions * Fries JF et al. Arthritis Rheum 1994;37:454-62 (modified)
the problem overlapping features example: systemic autoimmune diseases
systemic autoimmune diseases (1) examples • rheumatoïd arthritis • Sjögren's syndrome • systemic lupus erythematosus (SLE) • antiphospholipid syndrome (APS) • mixed connective tissue disease (MCTD) • systemic sclerosis (scleroderma, CREST-syndrome) • polymyositis / dermatomyositis • relapsing polychondritis
systemic autoimmune diseases (2) possible features • clinical • arthritis / arthralgia • vasculitis • fever • Raynaud's phenomenon • fatigue • various renal diseases • laboratory • increased ESR, CRP • anaemia • leukopenia • rheumatoid factor • ANA • trombopenia not specific for one single disease not specific for one single disease
systemic autoimmune diseases (3) possible accompaning organspecific autoimmune diseases • atrophic gastritis - pernicious anaemia • Hashimoto's disease • keratoconjunctivitis sicca • lymfocytic interstitial pneumonitis • myositis • pericarditis, pleuritis • peripheral neuropathy • uveitis (iritis, iridocyclitis) • scleritis • interstitial cystitis no combination is specific for one single disease
systemic autoimmune diseases (4) how do you recognize them ?
people how do you recognize them ? each person has a face
people how do you recognize them ? none of the parts of the face is unique, but the combination is
people how do you recognize them ? none of the parts of the code is unique, but the combination is
systemic autoimmune diseases (4) how do you recognize them ? each autoimmune disease has its own "face"
systemic autoimmune diseases (5) characteristic features characteristic feature specific way it affects the lacrimal and salivary glands specific way it affects the joints specific way it affects the skin specific way it affects the skin combination of clinical symptoms and anti-RNP specific way it affects the skin combination of symptoms disease Sjögren's syndrome rheumatoid arthritis systemic lupus erythematosus subacute cutaneous lupus erythematosus mixed connective tissue disease (MCTD) systemic sclerosis (scleroderma) CREST syndrome
characteristic features what are the characteristic features of IC ? • what is the consequence of the PBS/IC concept ? ICS definition of PBS/IC PBS: "suprapubic pain related to bladder filling, accompanied by other symptoms such as increased daytime and nighttime frequency in the absence of infection or other pathology" IC: above with "typical cystoscopic and histological features"
characteristic features what are the characteristic features of IC ? ICS definition of IC may be written as: suprapubic pain related to bladder filling, accompanied by other symptoms such as increased daytime and nighttime frequency with typical cystoscopic and histological featuresin the absence of infection or other pathology what are the "typical cystoscopic and histological featuresof IC" ? what has happened to urgency ?
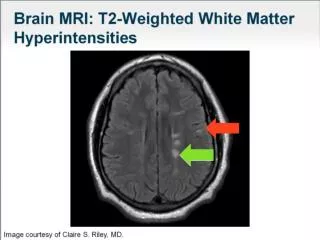
characteristic features what are the "typical cystoscopic and histological featuresof IC" ? • Cysto features: Hunner's ulcer or low capacity • epithelial denudation, submucosal inflammation, granulation tissue, edema, congestion, • haemorrhage; detrusor fibrosis (and myopathy) • increased mast cell number & activation and neuronal staining from: Hanno P, Burks D. Painful bladder syndrome / interstitial cystitis. Course 93 IC, AUA 2005 Annual Meeting, San Antonio, TX, May 21-26,2005
characteristic features • Cysto features: Hunner's ulcer or low capacity • epithelial denudation, submucosal inflammation, granulation tissue, edema, congestion, • haemorrhage; detrusor fibrosis (and myopathy) • increased mast cell number & activation and neuronal staining but these are not unique for IC ! from: Hanno P, Burks D. Painful bladder syndrome / interstitial cystitis. Course 93 IC, AUA 2005 Annual Meeting, San Antonio, TX, May 21-26,2005 does this matter as long as the combination is unique ?
PBS or IC IC IC has "typical" cystoscopic and histological featuresof IC in addition to suprapubic pain and frequency PBS / IC concept PBS
gold standard gold standard = diagnosis by experts why ? - the diagnosis by experts is the best standard we have as long as the cause of a disease is unknown advantage - non-experts can diagnose a disease as if they were experts (skill level) - diagnoses are made on the same basis by experts and non-experts (uniformity) - rules are based on information from many experts (acceptance and support)
classification methods (1) classification tree the classification tree is constructed by repeated splits of groups into 2 descendant subgroups Arthritis Rheum 1990;33:1137-44
classification tree • pro • items may be polychotomous or continuous • nonparametric: no reference to a model for the • relationship between classification items and disease • status • high information content - classified groups of subjects in • studies may be referred to the exact classifying subgroup • of the tree Arthritis Rheum 1990;33:1137-44
"number of criteria present rule" Ann Rheum Dis 2002;61:554-8
classification methods (2) "number of items present rule" • pro • simple definitions (+/-): easy application • con • simple definitions (+/-): • - all items are given equal weight • - all items must be dichotomous (+/-) • little insight into the characteristics of a • classified patient group Arthritis Rheum 1990;33:1137-44
suggested approach in a multicentre study 1. collect what information (symptoms and signs*) is used by experts to diagnose IC and differentiate IC from confusable diseases for both men and women * requires definitions and decisions on data format
suggested approach in a multicentre study 2. collection of data from patients with IC and patients with confusable diseases to define classification criteria for IC (training phase) sensitivity specificity calculate an optimal combination on the basis of how many false negative and false positive diagnoses we accept
suggested approach in a multicentre study 3. validation with new patient groups the same database can be used to create number of items present rule for clinical diagnoses and a classification tree for scientific studies
data format data may be - continuous avoid entry of cut-off points for continuous data but have the statistical analysis decide - categorical
to be evaluated …. tests to be evaluated for their diagnostic value should be done in all patients with IC and confusable diseases 1. antiproliferative factor 2. ................................ 3. ................................
summary & conclusions (1) 1. decision on broad definition of IC PBS + "typical" cystoscopy and/or histology 2. select diseases with which IC can be confused (confusable diseases, CD) list to be discussed this morning 3. what information is needed to distinguish IC from CD: follows from (2) but needs discussion and decision 4.decision onwhat percentage of false negative and false positive diagnoses we accept
summary & conclusions (2) 5. decision on gold standard for the diagnosis IC diagnosis by experts 6. decision on methods of classification classification tree and "number of items present rule" 7. decision to perform a small pilot to test procedures 8. decision on tests to be evaluated APF test