Download
1 / 32
350 likes | 813 Views
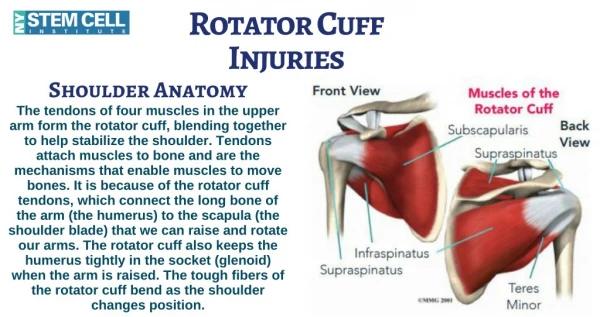
ARTHROSCOPIC ROTATOR CUFF REPAIR. T. Andrew Israel, MD Luther Midelfort Orthopaedic & Sports Medicine Center. OPERATIVE MANAGEMENT OF ROTATOR CUFF TEARS. Treatment Options Treatment Principles Surgical Indications Advantages of ARCR Disadvantages of ARCR Technique for ARCR Results.

E N D
ARTHROSCOPIC ROTATOR CUFF REPAIR T. Andrew Israel, MD Luther Midelfort Orthopaedic & Sports Medicine Center
OPERATIVE MANAGEMENT OF ROTATOR CUFF TEARS • Treatment Options • Treatment Principles • Surgical Indications • Advantages of ARCR • Disadvantages of ARCR • Technique for ARCR • Results
TREATMENT OPTIONS • ASAD/debridement without repair • Open repair • Mini-open repair • Arthroscopic repair
TREATMENT PRINCIPLES • Address associated pathology • Adequate decompression • Assess tear-size, retraction, pattern, tissue quality, repairability • Tendon mobilization • Secure repair • Supervised rehabilitation program
SURGICAL INDICATIONS • Pain • Functional deficits • Failure to respond to nonoperative care • Full-thickness tear • Extensive partial-thickness tear • Acute injury
ADVANTAGES OF ARCR • See both sides of cuff • Visualize all pathology-labral tears, biceps, OA, etc. • Easier releases(esp. capsule) • Less pain, morbidity • Smaller scars • Better ROM • PATIENTS WANT IT!
DISADVANTAGES OF ARCR • Learning curve • ? Smaller contact area with bone for healing • High retear rate by ultrasound reported • ? Pain from resorption of anchors • Coding/reimbursement problems
TECHNIQUE FOR ARCR • Define tear • Mobilize tendons • Prepare tuberosity • Cuff reduction • Place anchors • Suture management • Pass sutures through tear edge • Knot tying
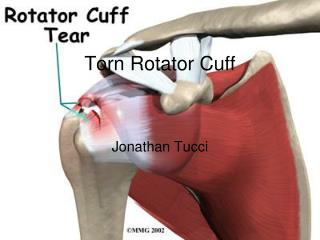
DEFINE TEAR • View from anterior and from posterior • Measure with probe known size • Trim ragged edges but preserve tissue
MOBILIZE TENDONS • Place retention sutures • Release capsule • Anterior interval release • Posterior interval release
PREPARE TUBEROSITY • Remove excrescences but preserve cortex • Trim tendon stump • Define footprint
MARGIN CONVERGENCE • Begin cuff reduction • Work medial to lateral • Side to side sutures • Tie knots
PLACE ANCHORS • At lateral aspect of footprint • Metal or biodegradable • Make sure well fixed in bone
SUTURE MANAGEMENT • Keep track of portals • Avoid tangles • Think one step ahead • Move at steady pace
PASS SUTURES THROUGH TEAR EDGE • Many devices available • Avoid tearing tendon • Line up puncture with anchor
KNOT TYING • Perfect knots • Perfect knots • Flawlessly perfect knots
RESULTS Gartsman, JBJS, 1998 • 73 arthroscopic RCR • Average age 60.7 yrs • All pts followed at least 2 yrs(30 mons) • 78% G/E relief of pain • 90% G/E satisfaction • None of the shoulders were rated G/E preop, 84% G/E @ most recent f/u
RESULTS Burkhart, Arthroscopy, 2001 • 59 arthroscopic RCR • Average follow-up 3.5 yrs • 95% G/E result regardless of tear size • Rapid return overhead function(4 mons)
CASE D.E. • 53 male RHD farmer • Left anterior shoulder pain x 2 years • No prior injury or surgery • Nonoperative Rx including PT, NSAIDS, injections, activity modifications, etc.
PHYSICAL EXAM • Crepitus with PROM • Tenderness greater tuberosity • AROM 155/170, 55/75, L5/T10 • 3/5 power abduction & external rotation • Positive impingement tests
SUMMARY • Much recent enthusiasm regarding complete arthroscopic rotator cuff repair • For many, this newer technique may be preferable alternative to more traditional mini-open rotator cuff repair • Important that basic principles of rotator cuff repair not be compromised
SUMMARY • Several short-term studies demonstrate excellent results comparable with those of traditional techniques • Choice of procedure based on variety of considerations, including patient expectations, pathoanatomy of the cuff, and arthroscopic skills of the surgeon