Download

1 / 47
470 likes | 1.18k Views
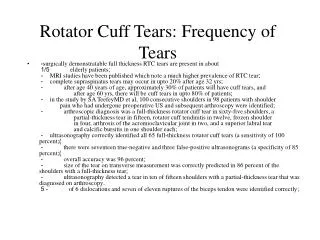
When to repair the rotator cuff?. Mr Simon Holland Ringwood Private Hospital www.simonholland.com.au. Take home messages. The rotator cuff has limited healing potential Untreated rotator cuff tears may result in cuff tear arthropathy Consider in all patients less than 60 y.o.

E N D
When to repair the rotator cuff? Mr Simon Holland Ringwood Private Hospital www.simonholland.com.au
Take home messages • The rotator cuff has limited healing potential • Untreated rotator cuff tears may result in cuff tear arthropathy • Consider in all patients less than 60 y.o. • Need a mobile shoulder
The rotator cuff has limited healing potential • The tendon typically tears in a hypovascular zone of the supraspinatus tendon • Poor blood supply = poor healing potential • Once a full thickness tear, the tendon retracts across the humeral head with minimal chance to adhere to this surface
Untreated rotator cuff tears may result in cuff tear arthropathy • This can be painful or painless • Often in patients with previous surgery • Difficult treatment options dependent on bone anatomy and pain • Treatment aims to maximize function vs loss of pain
Consider in all patients less than 60 y.o. • 60% of 60 year olds will have a rotator cuff tear on imaging • Most will will be asymptomatic • Most 70 year old rotator cuff tissue is of questionable quality
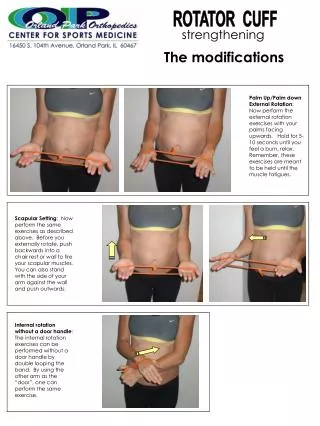
Need a mobile shoulder • A rotator cuff repair in a frozen shoulder is unlikely to be successful • Aim for passive range of motion • Physio - Jackin’s program • Hydrodilatation • Time • Surgical release
Case 1 • F53 Hairdresser self employed • Night pain, struggling with work (shoulder height) for 12 months • Failed physio • Good ROM • Weak SS (4/5) • Acromioclavicular joint non tender
Rotator Cuff Examination • Tenderness - tendon insertion, AC joint • If AC joint, ? cross arm or O’Brien’s aggravates • If posterior joint line, ? degenerative joint • ROM - exclude adhesive picture • Power (out of 5) • SS, IS, Subsc, Biceps
Imaging • Ultrasound (not particularly useful) • Suggested no tear, and patient delayed in presentation • Xrays - arranged - every patient • AP, true AP, Scapular Lateral and Axillary Lateral • Exclude other causes - OA, AC joint, fracture, cancer
Imaging MRI scans • When diagnosis is in doubt such as when pain is severe and patient wishes to know now, and not wait for time • Suspect multiple pathologies / limited equipment inventory • When third parties have an interest. Check and acknowledge other pain generators
Management Diagnosis • SS full thickness tendon tear Treatment Options • More of the same with subacromial cortisone injections • Surgical
Treatment Non Operative • Much research into why most tears are asymptomatic • EMG studies suggest poor subscap function in painful tears, but subscap directed treatment has not produced clinical nor EMG results • Equatorial theories - tear extends beyond a certain latitude, defunctioning the intact tendons
Treatment Operative Options • Subacromial Decompression • Rotator Cuff Repair • Acromioclavicular joint excision • Biceps Tenodesis
Subacromial Decompression • Arthroscopic or open • Assess coracoacromial ligament and undersurface of acromion • Smooth and débride • Resect subacromial bursa • Débride partial thickness tears of the undersurface(articular sided) of the rotator cuff
Rotator Cuff Repair • Arthroscopic, Open or Combination • Complete and incomplete • Anchors vs no anchors • Single vs double row repairs
Acromioclavicular Joint Excision • Often co-existing pathology • May contribute to SS impingement • Open or Arthroscopic
Biceps Tenodesis • Biceps often involved, especially with subscap tears where it subluxates and impinges against the coracoid process with adduction and internal rotation • Reattach or tenotomize • Can be trouble in its own rite
Principle Risks • Unintentional stiffness - compared to stabilization • Infection - < 1% for arthroscopic procedures • Repair failure, often asymptomatic • Healing of collagen is weakest at 4 months
Procedure • Overnight • Home exercise program • Analgesia and ice • Oxycontin, oxycodone/p. forte/digesic, NSAID • Sling for 6 weeks
Recovery • 0 - 10 days - standard exercises, keep away from work • 11d to 6 weeks - sling, light duties • 6 - 12 weeks - no sling, light duties • > 12 weeks - start to see a physio • > 6 months - aim for normal duties • 18 month before full recovery
Recovery • 0 - 2 weeks - will not think I am a friend • 6 weeks - suspect I have helped • 3 months - certain that I have helped and frustrated at the speed of healing • 6 months - about 90% when look back
Case 1 • Uneventful double row arthroscopic supraspinatus repair
Case 2 • M45, truck driver • Fall 2 months ago while unloading truck • Sudden pain, unable to lift away from body and not responding to non op measures • Smoker
Case 2 • Slight loss ROM • Tender - B, SS, Subsc • SS 4+. Subsc 3 (belly press), B 4 • Prominent AC, non tender
Case 2 US - aPTT of SS (hoped for a clue with biceps - need good ROM) XR and MRI • SS and Subsc FTT with Biceps Subluxation • AC arthropathy
Case 2 • 3 cm subsc tear, < 1 cm SS tear • Arthroscopic Subacromial decompression • Arthroscopic AC Joint excision • Open Subscap and SS repair with biceps tenodesis
Case 3 • F47 Office work • Fall in garden 8 months ago • Initially not able to actively move, sling for two weeks, gradual loss of movement • CSI of no value • NIDDM
Case 3 • Poor ROM and global cuff weakness 4/5 • Tender - general, AC • US - SS tear • XR - no OA
Case 3 • MRI - not going to change management. • Treat as adhesive capsulitis and when motion restored, reassess rotator cuff clinically and radiologically as indicated.
Case 4 • M35, sales representative • Mountain bike accident on single trail • ? dislocation, self reduced 6 weeks ago • Unable to elevate arm
Case 4 • Tender SS, posterior humeral head, anterior joint line • Full passive ROM, reduced active (< 60 FE) • Anterior laxity and positive apprehension signs • 3/5 SS power
Case 4 General Rule • 50% of those > 40 y.o. with a first time traumatic dislocation will have a rotator cuff tear. • Treatment is directed at the rotator cuff first and the instability second. • MRI is often helpful
Case 5 • M63, farmer • Longstanding ache that was at nuisance level for years, tripped at home and worsening pain and function • SS 4/5, IS 3/5
Case 5 Diagnosis = Massive Rotator Cuff tear • Xray to exclude fracture • Likely longstanding tear that extended. • Arthroscopic techniques offer less morbidity and better access to tendons • Discuss possible irreparable tendon
Case 5 • > 5 cm tear (massive) • Double row repair
Summary • When symptoms are more than a nuisance and non operative measures have been explored, surgical management and possible repair are viable treatment options.
Contact details: www.simonholland.com.au info@simonholland.com.au