Download
1 / 56
570 likes | 1.49k Views
KIDNEY DISEASES Developmental disorders Glomerular diseases Tubulo-interstitial diseases Urinary stones Obstructive uropathy Tumors. LUPUS GLOMERULONEPHRITIS GN-Common feature of SLE Immune complex-deposition -in situ formation Associated with deposits in -blood vessels

E N D
KIDNEY DISEASES Developmental disorders Glomerular diseases Tubulo-interstitial diseases Urinary stones Obstructive uropathy Tumors
LUPUS GLOMERULONEPHRITIS GN-Common feature of SLE Immune complex-deposition -in situ formation Associated with deposits in -blood vessels -tubular BM -interstitium Complementinflammation
LUPUS GLOMERULONEPHRITIS I: No lesion II: Mesangial III: Focal proliferative IV: Diffuse proliferative V: Membranous VI: Chronic
PATHOLOGY OF SLE GN • Highly variable • Immune complexes vary in/size/location • Subendothelial • Intramembranous • Subepithelial • Mesangial • Proliferation of Mes, End, Ep cells; PMN and MACROPHAGES • Fibrinoid necrosis • IF-”full house” (ML Ig)
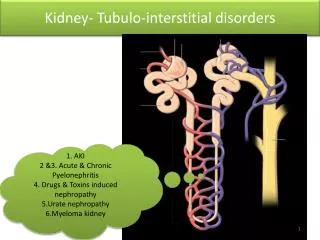
KIDNEY ANATOMIC COMPARTMENTS Glomerulus Tubules Blood vessels Interstitium Collecting system (Callices & Pelvis)
COMPONENTS OF THE GLOMERULUS • Capillary basement membrane • Mesangium • Bowman capsule • Cells • Endothelial • Epithelial • Mesangial
THE JUXTAGLOMERULAR APPARATUS Afferent arteriole Macula densa – ascending loop of Henle Lacis cells - Renin
CONGENITAL RENAL ANOMALIES Agenesis – Potter syndrome Ectopia Fusion Dysplasia Polycystic kidney disease
POLYCYSTIC KIDNEY DISEASE Autosomal dominant (adult) (1:1,000) Autosomal recessive (infantile (1:30,000) Medullary cystic disease complex (1:10,000) Medullary sponge kidney Acquired cystic renal disease
AUTOSOMAL DOMINANT POLYCYSTIC KIDNEY DISEASE Common kidney disease (1:1,000) 10% of all transplant/dialysis patients ADPKD-1 gene (polycystin) mutation 85% Bilaterally enlarged kidneys (>3,000g) Symptoms appear in adult life Renal failure 5-10 years thereafter
ADPKD Associated Conditions Liver cysts (30%) Splenic cysts (10%) Pancreatic cysts (5%) Cerebral aneurysms (20%) Diverticulosis coli
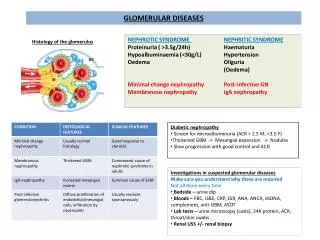
GLOMERULAR DISEASES Asymptomatic hematuria/proteinuria Nephrotic syndrome Nephritic syndrome Rapidly progressive glomerulonephritis Chronic nephritis
KIDNEY DISEASES (MNEMONIC “ANNURIC”) A Asymptomatic hematuria/proteinuria N Nephrotic syndrome N Nephritic syndrome U Urolithiasis R Rapidly progressive glomerulonephritis I Interstitial and tubular diseases C Chronic renal disease
CHRONIC RENAL FAILURE (UREMIA) General symptoms – weakness, fatigue Cardiovascular – hypertension, pericarditis G.I. – nausea, vomiting, diarrhea CNS – lethargy, confusion, coma Muscles – twitching, weakness Bones – osteodystrophy Metabolic – acidosis, PK, BUN, Cr. Endocrine - parathyroids
NEPHROTIC SYNDROME Proteinuria (“nephrotic range” >3.5g/24h) Hypoalbumimenia Edema Hyperlipidemia Lipiduria
CAUSES OF NEPHROTIC SYNDROME DiseaseChildren(%) Adults(%) Minimal change GN 75 20 Membanous GN 5 40 MPGN I 5 5 Other GN 5 20
NEPHRITIC SYNDROME Hematuria Proteinuria Hypoalbuminemia Oliguria (GFR, Cr, BUN) Edema (salt and water retention) Hypertension
DIAGNOSTIC FEATURES OF GLOMERULAR DISEASES • Light microscopy • Cellularity • Extracellular matrix • Special stains • (PAS, amyloid) • Immunofluorescence microscopy • (Linear, granular, mesangial, irregular deposits) • Electron microscopy • (deposits of immune complexes, BM changes, amyloid)
MINIMAL CHANGE GLOMERULOPATHY Most common cause of nephrotic syndrome in children E/P: unknown (?immune) Path: normal by LM and IF EM: fusion of foot processes CL: Nephrotic sy – responds to steroids Dd: FGS
FOCAL SEGMENTAL GLOMERULOSCLEROSIS Def: 15% of all nephrotic syndromes; heterogenous group of diseases E/P: unknown-circulatory glomerular injury (?) HIV, I-V drug abuse CHD, obesity, sickle-cell disease Path: focal and segmental glomerular hyalinosis “Collapsing” pattern (e.g. HIV) Trapping of serum proteins (IF and EM) Clin: Nephrotic syndromeESKD (5-20y) If HIV relatedESKD (1 year)
MEMBRANOUS NEPHROPATHY Def: Most common cause of nephrotic syndrome in adults (40%) Immune complexBM thickening E/P: Primary (unknown) Secondary (SLE, HBV, drugs, cancer) Path: Subepithelial deposits of immune complex CL: Nephrotic syndrome (25% recover, 50% persist, 25% progress)
DIABETIC GLOMERULOSCLEROSIS Def: Diabetes caused BM thickening Proteinuria renal failure (leading cause in US) E/P: BM synthesis , nonenzymatic glycation (?) Path: Diffuse global thickening of BM Nodular sclerosis (K-W) Arteriolosclerosis Trapping of serum proteins Clin: Proteinuria (in 50% diabetics) ESKD (30% all in the US)
DIABETIC KIDNEY DISEASES Glomerulosclerosis Arteriolosclerosis Hypertension Pyelonephritis Papillary necrosis
AMYLOIDOSIS AA amyloid – systemic disease AL amyloid – multiple myeloma Deposits of amyloid – glomeruli (mesangial) - arterioles - tulular BM Nonselective proteinuria – nephrotic sydrome (60%) renal failure (with large kidneys!)
ACUTE POSTINFECTIOUS GN Def: Acute nephritic syndrome 1-2 weeks after infection E/P: immune response to A -hemolytic streptococci (other infections Staph, malaria, HBV less common) Path: Acute glomerulonephritis Clin: Childhood nephritic syndrome 90% recover 9% presistent hematuria/proteirunria 1% chronic renal disease
PATHOLOGY OF ACUTE POSTINFECTIOUS GN LM: hypercellularity (endo + MES + PMN) IF: Irregular deposits of Ig, Compl. EM: Deposits (mesang + BM) “HUMPS”
MEMBRANOPROLIFERATIVE GLUMERULONEPHRITIS • Type I • Def: Immune mediated presistent GN • Mesangiocapillary cell proliferation and BM reduplication • E/P: Immune comples deposition in glomeruli • Primary (unknown cause) • Secondary (SBE, chronic infection, HCV, cryoglobulinemia, cancer) • Path: Lobular gromerulonephritis • Clin: Older children/young adults • Nephritic or nephrotic syndrome • Progressive – 50% ESKD (10 years)
MEMBRONOPROLIFERATIVE GLOMERULONEPHRITIS Type II Def: Immune mediated persistent GN Dense deposits in GBM E/P: C3 nephritic factor (IgG) Stablizes the activated C3 convertase Path: Similar by LM to MPGN-I EM-shows linear dense deposits in GBM
RENAL BIOPSY IN SLE To determine 1. Category (class) 2. Activity 3. Extent 4. Chronicity Note: Class IV-worst prognosis Class V-no response to steroids
IgA NEPHROPATHY (BERGER) Most common form of GN Young adults (15-30 years) Pathology: IgA deposits in mesangium -varied severity Clin: Protean manifestations 40% asymptomatic microscopic hematuria 40% bouts of macro hematuria 10% nephrotic syndrome 10% renal failure
ANTI-GBM ANTIBODY GN RPGN mediated by antibody Antibody to collagen IV Linear IF Fibrinoid necrosis of GBM Crescentic GN Goodpasture syndrome
CRESCENTIC GLOMERULONEPHRITIS • Anti-GBM glomerulonephritis • (inc. Goodpasture syndrome) • 2. ANCA granulonephritis • (inc. Wegener granulomatosis, micr. polyangitis, Churg-Strauss syndrome) • 3. Immune complex glomerulonephritis • (inc. Henoch-Schonlein purpura, cryoglobulinemia) • 4. Non-immune
ANCA GLOMERULONEPHRITIS Necrotizing and crescentic ANCA (PMN myeloperoxidase, proteinase 3) No immune deposits in glomeruli Respond to immunosuppresion (25% pregress) Associated with small vessel polyangiitis (75%) Pulmonary-renal vasculitic syndromes
SMALL VESSEL VASCULITIS AFFECTING KIDNEYS Henoch-Schonlein purpura-children, IgA Cryoglobulinemic vasculitis-HCV, MPGN-I Wegener GR.-upper slower respiratory tract Churg-Strauss-eosinophilia, asthma Microscopic polyangiitis-multiple organs, lungs (-)
NEPHROSCLEROSIS Benign – sustained mild hypertension – hyaline arteriolosclerosis – arterial fibrosis – glomerular hyalinization, tubular atrophy Malignant-BP>125 mm/Hg, retinal hemorrhage, papilledema, renal dysfunction – fibrinoid necrosis of arterioles – myxoid intimal expansion of arteries – microthrombi
THROMBOTIC MICROANGIOPATHY Morphologic finding in several diseases Assoc: microangiopathic hemolytic anemia E/P: HUS TTP Malignant nephrosclerosis Systemic sclerosis
RENAL INFARCTS • Thromboemboli • Mural thrombi • (M.I., atrial fibrillation) • Endocarditis • Aortic thrombi (atherosclerosis) • Cholesterol emboli
RENAL CORTICAL NECROSIS • Cortical ischemia: thrombi, vasospasm • Complication of shock • Abruptio placentae • Endotoxic shock • Hypotensive shock • Cortex pale – medulla spared • Massive tubular necrosis
CAUSES OF ACUTE TUBULAR NECROSIS • Ischemia (hypoperfusion) • Hypovolemic shock (e.g. bleeding) • Sepsis • Burns • Prolonged surgical operations • Nephrotoxins • Toxic chemicals (e.g. CCl4) • Heavy metals (e.g. Hg) • Drugs (e.g. cisplatin) • Heme proteins • Myoglobin (e.g. rhabdomyolysis) • Hemoglobin (e.g. hemolysis)
PATHOLOGY OF ACUTE TUBULAR NECROSIS Cortex> medulla Necrotic tubular cells slough off Intratubular cast in medulla Regeneration of tubules occurs fast
CLINICAL ASPECTS OF ATN • The most common cause of acute renal failure • “Dirty” brown casts in urine • Oliguria anuria polyuria • Azotemia • Acidosis, K • Fluid retention • Recovery 1-2 weeks
ACUTE PYELONEPHRITIS Bacterial infection (E. coli 80%) Ascending > hematogenous Lower UTI precedes renal infection Fever, flank pain, neutrophilia Leukocyte casts in urine Healing - recurrence chronic pyelonephritis
PATHOLOGY OF ACUTE PYELONEPHRITIS Unilateral> bilateral Focal PMNs in tubules interstitium Abscesses with tissue destruction
PYELONEPHRITIS PREDISPOSING CONDITIONS Urinary stones Hydronephrosis Cystitis Prostatic hyperplasia Tumors Pregnancy Vesico-ureteric reflux External ureteric compression (e.g. fibrosis)
PREDISPOSITION TO PYELONEPHRITIS (MNEMONIC URINE) U Urolithiasis R Reflux (vesico-ureteric) I Infections of lower UT N Neoplasms (e.g. ureteric, vesical, prostatic) E External compression (e.g.) pregnancy retroperitoneal fibrosis
CHRONIC PYELONEPHRITIS • PATHOLOGY • Destruction of renal tissue and fibrosis • Cortical scars • Loss of papillae • Ectasia of calices • Hydronephrosis • Irregularly shrunken small kidney • Histology: Chronic inflammatory infiltrates • Tubular atrophy with casts • (“thyroidization”)
DRUG INDUCED RENAL DISEASES • Acute tubular necrosis(toxic) • Acute tubulointerstitial nephritis (allergic) • Analgesic nepropathy (phenacetin dose-related)
METABOLIC TUBULAR INJURY Multiple myeloma – light chain casts Hyperuricemia (gout) – urate nephropathy Hypercalcemia – uric acid stones Hypercalciuria – nephrocalcinosis – calcium stones
CAUSES OF HYPERCALCEMIA – HYPERCALCIURIA • Primary (increased intestinal absorption of Ca) • Idiopathic (most common) • Milk-alkali syndrome • Vitamin D excess • Sarcoidosis • Secondary (release of Ca from bones) • Renal osteodystrophy • Hyperparathyroidism • Osteolytic metastases (e.g. breast cancer) • Paraneoplastic syndromes (PTrP)
RENAL STONES (NEPHRODITHIASIS) • Calcium oxalate or phosphate (75%) • Uric acid (15%) • Struvite (magnesium ammonium phosphate) • and calcium phosphate (8%) • 4. Cystine (1%)