Download
1 / 25
340 likes | 974 Views
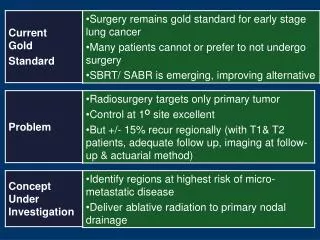
Kidney- Tubulo -interstitial disorders. 1. AKI 2 &3. Acute & Chronic Pyelonephritis 4. Drugs & Toxins induced nephropathy 5.Urate nephropathy 6.Myeloma kidney. Acute Kidney Injury (Acute Tubular Necrosis). Most common cause of Acute Renal Failure (ARF)

E N D
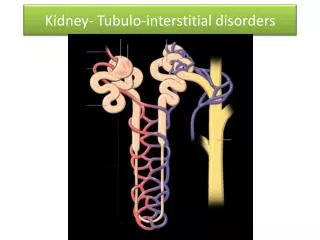
Kidney- Tubulo-interstitial disorders 1. AKI 2 &3. Acute & Chronic Pyelonephritis 4. Drugs & Toxins induced nephropathy 5.Urate nephropathy 6.Myeloma kidney
Acute Kidney Injury(Acute Tubular Necrosis) • Most common cause of Acute Renal Failure (ARF) • Acute reduction in renal function with tubular injury • Two types: • Ischemic • Toxic • Rapid reduction of renal function & urine flow-falls within 24 hrs to < 400mL / day. What causes AKI? 1. Ischemia: • Malignant Hypertension • Microscopic polyangitis • DIC • Hemolytic Uremic Syndrome (HUS). • Thrombotic thrombocytopenic purpura(TTP). 2. Direct Toxic Injury- Drugs like Gentamycin; radiographic contrast dyes ; Hg; CCl4 3. Acute TubulointerstitialNephritis - hypersensitivity reaction to drugs. 4. Urinary obstruction-tumors, BPH, blood clots.(Post renal causes)
AKI Ischemic Nephrotoxic Drugs: Gentamycin Radigraphic contrast agents Poisons & Heavy metals –Hg Organic solvents-CCl4 • Severe trauma; acute pancreatitis …. anything that causes inadequate blood flow to peripheral organs, accompanied by marked hypotension & shock. Ischemic & Nephrotoxiccombined: • Mismatched blood transfusions & other hemolytic crises-hemoglobinuria • Skeletal muscle injuries-myoglobinuria • Characteristic Hg & Myoglobin tubular casts .The IRON in these is toxic and causes AKI.
Fractional excretion of sodium - FENa • To clear a volume of plasma, the substance in that volume MUST be excreted (after filtering). The higher the % of the substance reabsorbed in the tubules,the smaller the volume of plasma cleared. • FENais not a test, but rather a calculation based on the concentrations of sodium and creatinine in the blood and urine.Urine and blood chemistry tests are necessary to perform this calculation. • The fractional excretion of sodium (FENa) measures the percent of filtered sodium that is excreted in the urine. This calculation is widely used to help differentiate prerenaldisease (decreased renal perfusion) from acute tubular necrosis as the cause of acute kidney injury (AKI). • FENa < 1% -Pre renal causes –eg. volume depletion • FENa > 1% -Renal cause – eg. ATN/AKI or interstitial nephritis.
ATN or AKI -2 Types Ischemic: • Discontinuous ,focal involvement at multiple points. • Tubulorrhexis. • Tubular lumen- casts-both hyaline & pigmented granular casts - Tamm-Horsfall protein. • Regeneration –is complete. Toxic: Mercuric chloride,CCl4 • Continuous – mainly PCT. • No B.M rupture.
Acute tubular necrosis. Casts Swollen ,vacuolated lining cells
Clinical course of AKI. 1. Initiation phase- lasts 36 hrs.-dominated by the cause ie, the inciting medical, surgical or obstetric event. Slight ↓ in renal output with ↑ BUN. 2. Maintenance phase: sustained ↓ in renal output- 40-400mL/day (oliguria), salt & water overload, ↑ BUN concentrations, hyperkalemia, metabolic acidosis, uremia. *maintenance of balance of water & electrolytes - crucial in this stage; Dialysis. 3.Recovery Phase: steady ↑ in urine volume up to 3L/day . Loss of water & electrolytes in the urine due to tubular damage. Hypokalemia. Eventually tubular concentrating ability returns. Takes time; but recovery is complete- depending on the initiating cause. *In shock related to sepsis, burns etc - 50% mortality.
Types of Tubular Casts. RBC Casts
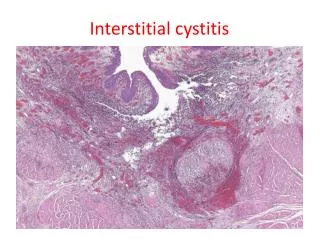
Tubulointerstitial Nephritis. 1. Acute & Chronic Pyelonephritis. 2. UTI-Urinary tract infection Vesicoureteric reflux Intrarenal reflux. In the absence of VUR, the infection remains in the bladder-cystitis & urethritis.
Both poles of kidney • *Self study- p.939-Etiology & Pathogenesis. • Endogenous infection • Catheterisation • UT obstruction& stasis of urine. • Incompetent V-U valve • Intrarenal reflux UTI-routes of infection-p 939-940 Voiding Cystourethrogram-Vesico-ureteric reflux *Self study- p.939-Etiology & Pathogenesis. Endogenous infection Catheterisation UT obstruction& stasis of urine. Incompetent V-U valve Intrarenal reflux
Acute Pyelonephritis(renal lesion associated with UTI) *Hallmarks: • Patchy interstitial suppurative inflammation. • Neutrophil aggregates in the tubular lumen • Tubular necrosis. *Secondary to bacterial and viral infections . *Polyoma virus - in renal allograft recipients - due to immunosuppression. Complications: • Papillary necrosis • Pyonephrosis • Perinephric abscess Healing is by scarring. The pyelonephritic scar is almost always associated with inflammation, fibrosis,& deformation of the underlying calyx & pelvis. *Self study- p.939-Etiology & Pathogenesis & p 942-Clinical features.
Grey white areas on cortical surface-abscesses Acute inflammatory cells within tubules & interstitium Healing-by scarring Polyoma virus-intranuclear inclusions.
Papillary necrosis. Tips of the pyramids show necrosis. Grey white to yellow necrosis-arrows. Papillary necrosis is also seen in: Diabetes Analgesic nephropathy Sickle cell disease Urinary tract obstruction
Clinical presentation: • Sudden onset.Pain at the costo vertebral angleSystemic: fever, malaiseDysuria, frequency, urgencyUrine:Pus cells++Leucocyte(pus)Casts- indicate renal involvement. WHY ? • Diagnosis: urine culture
Chronic Pyelonephritis –Read p 942 • Clin: back pain, fever, frequent pyuria, bacteruria. 2 Types: • Chronic Reflux-associated • Chronic Obstructive. • A rare variant is : *Xanthogranulomatous pyelonephritis characterized by the presence of: • Foamy macrophages • Plasma cells and lymphocytes, PMN • Giant cells • Proteus infection is common *Gross yellowish-orange nodules -D/D RCC • Chronic inflammation of tubules, interstitium, with extensive scarring. Involvement of *calyces and pelvis . • Condition can be bilateral • Asymmetric irregularly scarred kidneys (Contrast with Chr.GN) Microscopically: Atrophic glomeruli or, Normal with periglomerularfibrosis. Atrophic tubules Tubular lumen containing secretions simulating thyroid gland and hence the name “thyroidization’ of kidney • Can develop FSGS later.
Hallmark of Chronic Pyelonephritis: Coarse, discrete corticomedullary scars overlying dilated, blunted calyces; flattening of the papillae. Irregularly, asymmetrically scarred kidneys
Chronic Pyelonephritis Chronic inflammatory cells in the interstitium ; tubular atrophy or dilatation; Fibrosis. Dilated tubules filled with colloid casts- “thyroidization”
Drugs & Toxins • Drugs and toxins can produce renal injury in 3 ways: • Trigger interstitial immunologic reaction eg. acute hypersensitivity reaction by methicillin. • ARF • Subtle, cumulative effect—over yrs—CRF. Pathogenesis: IgE –mediated immune response may be involved in some. In others, Type IV-granulomatous reaction Drugs act as haptens + bind to cells = become immunogenic. Drugs: • Sulfonamides • Methicillin, ampicillin • Rifampicin • Thiazide diuretics • NSAIDS • Allopurinol • Cimetidine Clin: Fever, skin rash, eosinophilia, renal abnormalities - about15 days after taking the drug. A rising S Creatinine level or ARF with oliguria – in 50 % cases. Synthetic
Acute drug-induced interstitial Nephritis. • Interstitium-edema • Infiltration by lymphocytes, macrophages. • Eosinophils & neutrophils may be seen in clusters. • Plasma cells, basophils-small number. • Glomeruli - normal; except sometimes in NSAIDS-minimal change & N.S develop. • Important to recognise, as withdrawal of the drug –causes reversal – but it takes time.
Analgesic Nephropathy.* Phenacetin • Was one of the leading causes of end-stage renal disease in Australia & other countries until public health measures reduced the sale of over-the-counter medications containing these mixtures. • Due to excessive intake of analgesic mixtures containing Phenacetin, aspirin, caffeine & codeine. Acetaminophen depletes cells of glutathione, then injures cells by generation of oxidative metabolites. • More common in women & in people suffering from psychoneurotic illness; recurrent headaches & muscle pain. • Causes papillary necrosis first and tubulointerstitial nephritis next. Papillae may be sloughed off in to the urine. • Complications include the development of transitional cell carcinoma of the renal pelvis in a small% of patients. Papillary necrosis-in varying stages of damage. Gross hematuria or renal colic
Nephropathy associated with NSAIDS. Aristolochic Nephropathy. • Uncommon, but should be kept in mind. • The selective COX-2 inhibitors, while sparing the GIT, may damage the kidneys. • ARF-↓synthesis of vasodilatory PGs • Acute hypersensitivity interstitial nephritis -ARF • Acute interstitial nephritis & MCD - ?hyprsensitivity reaction ? Or, cytokine mediated injury to podocytes? • Membranous Nephropathy with the N.S- ? unclear • Aristolochic acid is found in certain herbal medications. • The drug forms co-valent adducts with DNA & causes a distinctive picture of renal failure & interstitial fibrosis; associated with a relative paucity of infiltrating leukocytes. • ↑ incidence of carcinoma in the kidney & urinary tract. • Also the cause of Balkan nephropathy.
Urate Nephropathy. • Acute uric acid nephropathy shows crystals in the tubules (acidic pH in C.Ds) – obstruction and renal failure; seen in patients who are on chemotherapy for leukemias; lymphomas. • Chronic urate (Gouty) nephropathy (Gout-1243-6)- with hyperuricemia – deposition of monosodium urate crystals in the acidic distal tubules & CDs. • Birefringent needle-like crystals in tubular lumen or interstitium. • Nephrolithiasis – presence of uric acid stones – found in gout and secondary hyperuricemia. Giant cell reaction & fibrosis around the crystals.
Light-chain cast Nephropathy/Myeloma Kidney • Bence Jones proteinuria & cast nephropathy. • Tubular casts- combination of Bence Jones protein &Tamm-Horsfall protein-obstruct the tubular lumina; induce inflammatory reaction around the casts. • Amyloidosis- AL type. • Casts-pink to blue amorphous masses, fill & distend the lumen. Giant cell reaction.