Download

1 / 71
710 likes | 892 Views
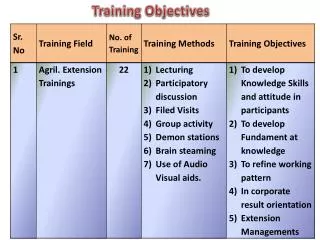
Training Objectives. To understand the current recommendations on infant safe sleep practices To understand the barriers to following safe sleep recommendations To learn techniques for how to work effectively with parents to increase safety. Definition of Sudden Infant Death Syndrome.

E N D
Training Objectives • To understand the current recommendations on infant safe sleep practices • To understand the barriers to following safe sleep recommendations • To learn techniques for how to work effectively with parents to increase safety
Definition of Sudden Infant Death Syndrome “The sudden and unexpected death of an infant under one year of age, with the onset of the lethal episode apparently occurring during sleep, that remains unexplained after a thorough investigation including performance of a complete autopsy, review of the circumstances of death and the clinical history.”
Leading cause of infant deaths from 28 days to 1 year. 85% of all sudden and unexpected infant deaths between the age of 1 month and 1 year are due to SIDS. Highest incidence occurs between 2 to 4 months. 90% of SIDS occur from 1 to 6 months of age. Higher incidence among male infants. Facts about SIDS
Maternal Risk Factors • Smoking during and after pregnancy • Maternal age < 20 years • Poor prenatal care • Low weight gain • Anemia • Use of alcohol or drugs • History of STDs or UTIs
Infant Risk Factors • Male • Low birthweight • Premature • African-American • Native American • Exposed to tobacco and drugs
External Stress Factors (Modifiable) temperature swaddling bedding sleep position smoking drug use minor respiratory symptoms poverty limited prenatal care season Triple Risk SIDS Theory Vulnerable Infant SIDS Critical Development Period External Stress Factors • (age – vulnerability) • 2-4 months - 75% • 4-6 months - 15%
Current Theories Based on Recent Research Cerebral Cortex • Chemical receptors that respond to low blood oxygen or high blood carbon dioxide may not function normally • This could lead to respiratory failure and death in certain circumstances • Prematurity, exposure to cigarette smoke and other risk factors may operate by contributing to this abnormal function Brain Stem
Environmental Risk Factors Prone sleeping (sleeping face down) Is estimated to account for 40-80% of SIDS cases Source: Nursing Research Mar/Apr 2004
Back sleepers who nap on their tummies face an 19-fold risk of SIDS. Source: Mitchell and Thach, Arch Pediatr Adol Med, 1999 Tummy sleepers are 5 to 7 times at greater risk of dying of SIDS thanback sleepers.
Environmental Risk Factors Overheating
Sleeping in Adult Beds Can Result in: • Entrapment/wedging • Overlying • Suffocation from Bedding • Strangulation
Comparison of Risk for Suffocation in Adult Bed and Sofa/Chair • For infants younger than 8 months, risk of dying in a crib was 0.63 deaths per 100,000 infants • Risk of dying in adult bed was 25.5 deaths per 100,000 infants Source: Scheers, et. al., “Where Should Infants Sleep? A Comparison of Risk for Suffocation of Infants Sleeping in Cribs, Adult Beds, and other Sleeping Locations,” Pediatrics Vol. 112 No. 4 October 2003
The Incidence of Bed-sharingIt’s on the Rise The incidence of bed-sharing has increased from 5.5% in 1993 to 12.8% in 2000. Source: Archives of Pediatrics and Adolescent Medicine, January 2003 Source: National Infant Sleep Position Study
What are the Reasons Given for Bedsharing ? • No crib 2. Easier to breastfeed at night • To avoid crib death • Family tradition 5. To spend quality time 6. Too tired to get up • To keep baby warm • Baby sleeps better
PANHANDLE FIMR STUDY OF SLEEPING INFANT DEATHS from 1994-2003 87% (46/53) of cases had one or more documented “sleep risk factors”: Placed on adult bed (50%) Placed on sofa, chair, pillow of lap (22%) Positioned on stomach (55%) Slept on or near questionable bedding (74%) Slept with other family members (56%) Exposed to second-hand smoke (30%)
AAP Recommendation for SIDS Risk Reduction A separate but proximate sleeping environment is recommended
What Are The Barriers To Following Safe Sleep Recommendations?
National Infant Sleep Position Study • National annual telephone survey or 1000 households • African American. Hispanic, Asian and American Indian parents of 2 and 4 month olds
Findings from Focus Groups with Caregivers Caregivers reported concerns about: Safety – choking Comfort – believed child more comfortable on stomach Advice – trusted family members and their own instincts over health professionals
Findings from Focus Groups with Caregivers Caregivers lacked knowledge about: What causes SIDS The dangers of soft bedding Why back sleeping is important
Why are Parents Still Putting Babies to Sleep on Their Stomachs? • Baby sleeps better on stomach • Baby cries if put down on his back • Baby will choke • Baby can breathe easier • Advice from grandmother • Previous experience • Doctor said it was ok
Preemies No Longer Exempted Based on all available data, we now recommend that all full-term and preterm infants in the NICU without upper airway obstruction be placed in the supine position for sleeping as soon as ready for oral feedings. Dr. Carl Hunt
American Journal of Maternal Child Nursing • 55% Side • 16% Prone • 29 % Supine Nov/Dec 1999, Infant Sleep Positioning: Nursing Practice and Knowledge, Peek Hershberger, Kuehn and Levett
Tasks of Falling Asleep • Regulating sleep-wake cycles • Internalizing daily routines and schedules • Transitioning from active and quiet alert states to sleep • Screening out noise to fall asleep • Self calming when awakened in the night • Feeling attached to caregivers while feeling secure in separating from them to sleep Source: Pediatric Disorders of Regulation in Affect and Behavior. De Gangi. 2000
Sleep Problems • Difficulty initiating (settling into sleep) • Difficulty maintaining sleep (waking up during the night with difficulty returning to sleep Source: Diagnostic Classification 0-3
Causes of sleep problems • Medical Problems • Regulatory Disorders • Attachment Disorders • Poor Sleep Hygiene
Medical Problems Which Interfere With Sleep 1. Obstructive sleep apnea syndrome (OSAS) • Respiratory conditions, e.g. asthma, CF • Food allergies • Ear infections
What Is Self Regulation? “The mastery of tasks that were accomplished by the mother’s body or in concert with the mother’s body when the child was in the womb, but must now be accomplished by the child’s body and through signaling needs to responsive adults.” Source: From Neurons to Neighborhoods, 2000.
Developmental Milestones of Self Regulation In Infancy • Regulation of arousal and sleep-wake cycles • Responsive interactions with others • Attempts to influence others • Begins to anticipate and participate in simple routines Source: Bronson, Martha. (2000). Self Regulation in Early Childhood. New York: Guilford Press.
Role of Adults in Infant Self Regulation • Being sensitive to infant signals and “state” • Being responsive to infant’s signals • Engaging in warm positive interactions • Participating in predictable sequences of caregiving, social and play routines that the infant can learn and participate in Source: Bronson, Martha. (2000). Self Regulation in Early Childhood. New York: Guilford Press.
Sleep Problems Occur in Children with Regulatory Disorders • Hypersensitive Over-reactive to touch or sound Difficulty settling or getting comfortable • Motorically Disorganized Craves vestibular stimulation Can only fall asleep with movement or vibration
Disorders of Attachment in Infancy Can Affect Self Regulation • Constitutional vulnerabilities in the infant • Emotional liabilities in the parents • Poorness of fit Source: Infant and Toddler Mental Health, edited by J. Martin Maldonado-Duran, M.D.
Are less active Are more irritable Show fewer positive expressions Have disturbed sleep patterns Have increased stress hormones Source: “Breaking the Cycle of Depression” American Psychological Association Newborns of Depressed Mothers
Poor Sleep Hygiene • Feeding a baby every time it cries • Parent soothing vs. self soothing
How Can We Help Parents to Implement Safe Sleeping Recommendations?
DEPRESSED MOTHERS ARE • Less likely to breastfeed • Less likely to use “back to sleep” position • Less likely to take child for recommended preventive care and immunizations • More likely to use corporal punishment Source: “Maternal Depressive Symptoms and Infant Health Care Practices Among Low Income Women” Chung, et. al., Pediatrics Vol. 113 No.6 June 2004
Give Back to Sleep Recommendations During Postpartum Hospital Stay • Ask about SIDS knowledge • Ask what recommendations they have heard • Ask if they know why side is not recommended • Ask if they are worried about choking • Ask what they think about the recommendations • Ask if they have questions