Download
1 / 52
570 likes | 1.98k Views
Internal and External Respiration Gas Transport Regulation of Respiration. Once we get the air into our lungs- we have to get the oxygen loaded onto the RBC and the CO 2 off the RBC Then reverse this process in the systemic capillary.

E N D
Internal and External RespirationGas TransportRegulation of Respiration • Once we get the air into our lungs- we have to get the oxygen loaded onto the RBC and the CO2 off the RBC • Then reverse this process in the systemic capillary. • Problem: Diffusion across cell membranes and gases coming into and leaving a fluid. Chapters 39-41, 44
Taken from Wikipedia; Adolf Fick Fick’s Law of Diffusion • Fick’s Law defines factors that influence diffusion Rate of Gas Diffusion= Surface Area x Pressure x Diffusion Coefficient Distance for diffusion where Diffusion Coefficient = Gas Solubility/(Gas Molecular weight)½
Pressure gradient comes from Gas Pressure • PV=nRT (Ideal Gas law) • Think of pressure as the number of collisions • IF one mole of helium= 100mmHg, what would the pressure be for 2 moles? • What if 1 mole of helium and add one mole of oxygen?
Air is a mixture of gas molecules • Dalton’s Law: The total pressure of a gas mixture = sum of the partial pressures of each gas; each gas contributes part of the total pressure. • Air ~ 79% N2 + 20.9% O2 + .03% CO2 • PATM = P total =PN2 + P02 + PCo2 = 760 mm Hg • P02 = 0.21 x 760 mmHg = 160 mmHg • P N2= 0.79 x 760 mmHg = 600 mmHg • PCO2= 0.0003 x 760= .23mmHG • We are assuming no humidity (pressure from water) PATM decreases with increasing altitude PATM increases with depth below sea level
An introduction to Henry’s Law Dealing With Problems of Gas Solubility Moving Gases Between Air/water O2 Equilibrium: gas molecules enter and leave the liquid at the same rate O2 Reminder: Alveolus = air space Capillary = water filled space capillary Alveolus
p O2 O2 Henry’s Law(the concentration of gas molecules in a liquid depends on two things. They are: The concentration of a gas in a liquid = pressure of the gas above the liquid x solubility of the gas in the liquid.) Concentration = pressure x solubility At equilibrium: gas molecules enter and leave the liquid at the same rate (that means there is equal pressure in the gas and liquid)
Gas filled chamber (think alveolus!) P gas above liquid Tray of water (think plasma!); gas is pushed into water at air/water interface P gas in the liquid Reminder: Alveolus = air space plasma = water Pressure and solubility • Gases differ in their solubility in water (CO2 is 24 times more soluble in water than is O2 and 20 times more diffusible) When comparing two gases, the gas that is less soluble will show a greater rise in partial pressure in the liquid
Pressure vs. Concentration • At equilibrium, the dissolved gas molecules and those in the gaseous phase are at the same partial pressure • Does this mean they are at the same concentration? • NO! • But, their concentration is proportional to the partial pressure (that is, if partial pressure goes up, then the concentration of that gas in the liquid will go up—they are directly related.) • So, what other factor determines the concentration of a gas in a liquid, if it’s not just pressure? • Well.......
PCO2= 100mmHg PCO2=100 SOLUBILITY [O2]air= 5.2mmole/L PO2= 100mmHg PO2= 100mmHg PO2=100 PO2=0 [O2]water= 0.15mmole/L What would happen to concentrations if the gas pressures were doubled? Look at these gases- they are at equilibrium, but notice the concentrations of the molecules are NOT equal [CO2]air= 5.2mmole/L PCO2= 100mmHg PCO2=0 [CO2]water= 3.0mmole/L
Nitrogen sickness The “bends” and Sodas • A perfect application of Henry’s Law • N2 is the predominant gas in air • It is only half as soluble in plasma as oxygen, so normally, hardly any dissolves in our plasma. • But underwater, at great depths, atmospheric pressure rises. (every 10 meters, increases by 760 torr) • N2 is forced into our plasma when we breath it, due to the high atmospheric pressures experienced underwater (deep sea diving) • N2 gas remains solubilized while underwater (think soda in a capped, pressurized bottle), not a problem. • When atm pressure is reduced, as when a diver surfaces too quickly, N2 gas comes quickly “out of solution” (think soda bottle uncapped.) Bubbles form in capillaries, and lodge in-place; block blood flow. Anoxia, cell death. • Treatment: hyperbaric chamber or submersion to depths.
Dave Shaw: Raising the Dead • Bushman’s Hole-South Africa • 3rd deepest freshwater cave • Deon Dryer • 270 meters/ 927 feet! • Roughly 9 hours to decompress • Saturation diving: usually helium and oxygen • Trimix- oxygen, helium, and nitrogen • At depth oxygen is toxic- seizures, disorientation at 4 atmospheres causes coma within 30-60 minutes • Nitrogen is a narcotic (martini affect-nitrogen narcosis) • Helium- muscle spasms • Deep water blackout from Carbon dioxide build-up—high CO2 causes depression of respiratory center instead of exciting it because of the negative tissue metabolic effects. August 2005 issue of Outside
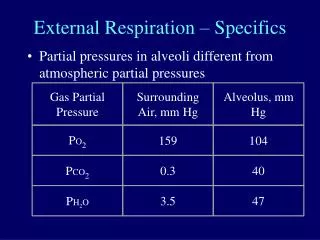
Alveolar and Blood Gases (mmHg or Torr) the amount of a gas that diffuses from the alveolar air into the capillary blood is dependent directly on the partial pressure of the gas driving it PN2 = 600 Patm = 760 PO2 = 159 PCO2= 0.3 Gases diffuse down their pressure gradients (Fick’s Law). How would the gases diffuse here? The rate of this only takes 0.25 seconds Partial pressures of gases represent the relative concentration of the gas. PN2= 573 PH2O= 47 PO2 = 100 PCO2= 40 PO2 = 100 PO2 = 40 PCO2= 40 PCO2= 46
Ventilation Perfusion Matching Lung Height Pleural membranes Visceral and parietal pleura Pleural space; pleural fluid
Ventilation Perfusion Matching V = ventilation Q = perfusion Lower regions receive more perfusion than ventilation (dependent regions, bottom of lung) = physiologic shunt Upper regions receive more ventilation than perfusion, = physiologic Deadspace air Fig 39-11 Lower Upper perfusion Q V ventilation
P alveolar P capillary P alveolar
Change in gas composition in lungs Response of Bronchioles Response of pulmonary arterioles Increased PCO2 Dilation( VA) Weak constriction ( Q) Decreased PCO2 Constriction ( VA) Weak dilation ( Q) Increased O2 Weak Constriction ( VA) Dilation ( Q) Decreased O2 Weak dilation ( VA) Constriction ( Q) Local control of Ventilation and Perfusion
Respiratory membrane pO2= 40 Torr pCO2 = 46 Torr pO2= 100 Torr pCO2 = 40Torr Pulmonary Capillary Transit time When diffusion is impaired, we need that reserve time to allow for diffusion to complete. For example when we exercise, our cardiac output increases, transit time decreases and reserve time is shortened! Transit time in lung capillary is ¾ of second. Diffusion occurs in the first ¼ second Allows ½ second for reserve time pO2 = 100 Torr pCO2= 40 Torr pH2O- 47 Torr pN2= 573 ¼ 2/4 ¾
If reserve time is shortened... • Now erythrocytes may leave the lung not fully loaded (saturated) with oxygen. • How will you know? Measure the patient’s arterial blood gases…. PO2, PCO2 - to tell if lungs are not delivering enough O2 to tissues- hypoxia. • Patient is asymptomatic (at rest) • Start stress test • Cardiac output goes up. HR always has to go up- time for diastole goes down and oxygen for the ventricle, too! • But pulmonary time is decreased- less time and less saturation of RBC, so amount of loading going onto the Hb will be fewer- maybe only 2 or 3. • Myocardium is hypoxic—arrhythmia or infarct may occur! Resting time? Perfusion? 3 out of 4 oxygen on Hb is needed! • Exercise stress tests demonstrates how much reserve is in patient- sees just how sub-threshold of disease pathology the patient is.
At rest, the avg person consumes 250 ml oxygen each minute. Can we deliver that much with our cardiac output of 5L/min? Oxygen delivery
O2 Transport in plasma Henry’s law: At 100 torr Plasma holds only 0.3 ml O2 / 100 ml plasma (concentration of O2) Think of this At rest, we consume about 250 ml O2 /min. If dissolved oxygen in plasma were the only way to carry oxygen, then at rest, we’d have to have a cardiac output of 83L/min to feed our tissues. Math: 0.3ml/100ml plasma x ?ml/min = 250ml/ min
Hemoglobin allows blood to hold more oxygen (It increases the oxygen “carrying capacity” of blood.) How much more? Well, it depends on how much Hb you have! Do you remember Hb concentration measurements from your first lab? Oxygen Transport in Blood: Plasma and RBCs
RBCs—sacks of Hemoglobin When fully saturated, Hb capacity for oxygen is: 1.34 ml O2/ gm Hb. Assuming a normal Hb concentration of 15 gm%, Hb carrying capacity is 20.1 ml O2 / 100 ml blood How many times greater is the carrying capacity of Hb than plasma? 67 times (= 20.1/0.3)
O2 Transport • Of course O2 transported both ways in the blood: • Dissolved in the plasma • Bound to Hb in RBC So the total oxygen transported in blood is the sum of both, add them together! 20.1 + 0.3= 20.4ml O2/100ml blood The loading and unloading reactions: Loading occurs in lungs; Unloading occurs in tissues. Deoxyhemoglobin + O2 Oxyhemoglobin Question: exactly HOW does this loading/unloading occur?
Hemoglobin • Large protein consisting of 4 polypeptides • 2 chains and 2 β chains • Each chain contains a single molecule of heme, an iron-containing pigment • Why not just use the heme group only? • The iron ion in heme is able to reversibly bind an oxygen molecule due to change in affinity caused by H+ and CO2 • Meaning, O2 can bind to Hb at the lungs and then be released at the tissues Note the 2 chains and 2 β chains. Notice how each has an associated heme molecule with an iron atom.
Iron • Obtained in the diet • Ferrous (reduced) form binds oxygen (+2) • Ferric (oxidized) for cannot bind oxygen (+3) • Hb with iron in ferric form is called methemoglobin
Pyrrole groups Protoporphyrin ring Porphyrin ring= bound iron; aka “heme” Globin Chains and Heme • Determine the affinity for oxygen • Embryonic Hb (HbE) 22 • Fetal (HbF) 22 • Adult (HbA) 22 • Different oxygen affinities • Are expression products of different genes • Products of different genes (chromosomes 11, 16) are expressed throughout life
Perhaps this is a new term? • Biochemical term • “affinity” • When two molecules bind, the tightness with which they bind to each other is termed “affinity” • Greediness (less tendency to let go) Which couple is “binding” with greater affinity? Rank them.
How do the globin chains determine affinity? Through allosterism • Definition: changes in one part of the molecule are communicated to other parts of the same molecule by changes in the molecule’s shape (conformational changes.) • Every time an O2 comes on, this will change the shape of other Hgb and make it easier to bind oxygen • Hb is a tetramer (4 subunits)
Allosterism • The sigmoid shape of the Oxy-Hb dissociation curve reveals allosteric interactions are occurring between the 4 subunits in any one Hb molecule. • Analysis of the slope of the curve reveals that Hb’s affinity for each of oxygen is not the same. • That is, when unloading oxygen from Hb, it is hardest to pull off the first oxygen (highest affinity when all 4 are loaded); easier with each successive unloading, but slightly harder again to unload the 4th oxygen. • Let’s talk allosterism with respect to children “leaving the nest.”
Sigmoid Curve hints at allosterism Something’s going on in each Hb molecule
Oxyhemoglobin curve • What does this graph tell you? • How saturated the Hgb is • If 100% saturated, then all the Hgb present is bound to O2 • What doesn’t this graph tell you? • If a patient is anemic. • A person with 12mg/100ml of blood is anemic, but would still be 100% saturated but the carrying capacity will be down!
Also keep in mind: • Blood gas measurements indicate the amount of O2 dissolved in the plasma. (dependent on ventilation and absorption by blood) • Partial Pressure • Depends on percentage of gas • Driving force for diffusion • They do not indicate the amount of O2 bound to the hemoglobin. • Saturation • % Hb that has oxygen bound (note: no units) • Content • Absolute quantity (ml O2/100 ml blood) • Carrying Capacity: O2 content at 100% saturation. • Anemia, Polycythemia • Hematocrit • Hemoglobin
Back to Allosterism But that’s not all…. • There is also communication between each globin chain and its heme group • Globin chains are rich in the a.a. histidine (imidazole group pKa, each one is capable of binding both a H+ and a CO2 molecule.) • When either of these bind, Hb’s affinity for oxygen decreases. (Bohr effect) And the reverse is true as well,… • When oxygen binds to Hb, Hb’s affinity for H+ and CO2 decreases. (Haldane effect)
Allosterism • This means that Hb’s affinity for oxygen is affected by pH and pCO2 of the plasma. • It is also affected by temperature (tighter in cold) • It is also affected by a substance in the erythrocyte known as 2,3 BPG (a product of anaerobic respiration) ACID!
This type of allosterism is revealed in “Shifting” the Hb Dissociation Curve • Curve shifts (left or right) • Shifts reflect changes in Hb’s affinity for oxygen. • Shift to left means Hb holds onto oxygen more tightly, “Hb’s O2 affinity increases” • Shift to the right means Hb holds onto less tightly, “Hb’s O2 affinity decreases” Be certain you can interpret this directly from the graph.
Four (+ one) Things Change Oxyhemoglobin Affinity • Hydrogen Ion Concentration, [H+] • CO2 Partial Pressure, pCO2 • Temperature • [2,3-DPG]
Shifts in affinity 2,3 DPG is a by-product of metabolism in the RBC. RBC undergoes an anaerobic Hexose monophosphate shunt to make ATP and 2,3 DPG is a by-product. When RBC is low in O2, it makes more 2,3 DPG- and this shifts the curve to the right. This is an internal regulator within the RBC.
HgbF vs. HgbA-actually really do have the same affinities, how do you explain this graph?
The special case of Carbon Monoxide (CO) • Gas, odorless, colorless, tasteless • You won’t know when you’re surrounded by it • It does not change your breathing rate, or give sensation of “air hunger” (dyspnea) • Binds to Hb at same site oxygen would bind: the iron atom. Displaces, or “competes” with oxygen (decreases Hb’s capacity to bind oxygen) • Hb’s affinity for CO compared to O2 is 210:1, in other words, Hb “prefers” CO over oxygen! • But yet, it shifts the Oxy-Hb curve to left, making any oxygen that is simultaneously loaded on the same Hb molecule remain more tightly bound (shift to left = higher affinity) Hb is less likely to release any oxygen it has to the tissues! Anoxia, cell death. • Meaning if one CO, but three remaining O2, this lowers saturation curve, and the affinity for O2 increases! • Blood still red! No signs! pO2 is normal!
Three Things That Change O2 -Carrying Capacity of Blood • Changes in Hb Concentration • Presence of Carbon Monoxide • Formation of Methemoglobin Shift to the left
What about CO2 Transport? CO2 is transported 3 ways in both the erythrocyte and in plasma: • “Hydrated” CO2 that is, chemically combined with water to form bicarbonate. (HC03-) This is due to action of carbonic anhydrase in the RBC. 70% • CO2 dissolved in water (“solubilized CO2”) either in plasma or inside the RBC. 10% • Carbamino compounds on proteins (albumin in plasma, Hb in RBC.) 20% Hgb. CO2 Hgb carbonic anhydrase CO2 H2O +CO2 H2 CO3 HCO3- + H+ H++Hgb- HHgb CO2 Cl- HCO3-
The Chloride Shift: Cl- is exchanged for each HCO3- Haldane effect in lungs: oxygen displaces carbon dioxide
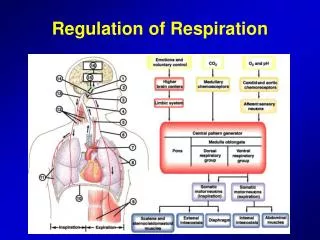
Regulation of Respiration • Feedback and Homeostasis (setpoint) • Sensors • Receptors gather information; send AP’s to report on blood/CSF chemistry • Central controller • integrate incoming signals (summation of AP’s) in medulla and pons • Effectors • Signal muscles of respiration to contract
Respiratory Centers: Medulla oblongata and Pons • (Pneumotaxic Center: modifies inspirations, • increase respiratory rate • Medulla • Dorsal respiratory group • inspiration, intrinsic nerve activity; ramping of AP’s • Ventral Respiratory Group • Inactive during quiet respiration • Active during forced respiration Figure 41-1; Guyton & Hall
Chemoreceptors • Carbon Dioxide, Hydrogen Ions • Central chemosensitive area of medulla; senses levels in CSF • Oxygen • Peripheral chemoreceptors; sense levels in blood • Aortic chemoreceptors (CN X) • Carotid chemoreceptors (CN IX) • responds to oxygen (greatest Po2<100 mmHg)
CO2 CO2 Chemosensitive Area of Respiratory Center Figure 41-2; Guyton & Hall Brain Tissue CSF Blood low protein pH=7.32 PCO2=50 blood-brain barrier chemoreceptor H+ H+ Via CA CO2
Regulation of breathing • Blood PO2 does not change rapidly in response to changes in ventilation because of the large reservoir of O2 bound in RBCs. • Because of this changes in PCO2 act as the most important stimulus for control of ventilation. • Usually resp increases 2-3 x for every 3mmHg of CO2 • If hypoventilation occurs, PCO2 rises (hypercapnia) and blood pH falls. • If hyperventilation occurs, PCO2 falls (hypocapnia) and blood pH rises.
Periodic Breathing “My every waking breath shall be my pledge of love to you.” • Cheyne-Stokes Breathing • Stroke Brain trauma turns off respiratory drive for few seconds • CO2 levels turn it back on with force! • (increased negative feedback gain). • Ondine’s Curse (Congenital Central Hypoventilation Syndrome) • 400 sufferers worldwide • Thox2B gene (May 2003) • Central Sleep Apnea Undine with harp by Ludwig Michael von Schwanthaler (1855)
Clinical consideration • In the normal person, it is the rising level of CO2 (plasma pCO2) between each breath that is major stimulus to ventilate … it drives one’s “need” to inhale. (“air hunger”/ dyspnea) • Acts on central chemosensitive area through pH • In times of chronic hypercapnia and respiratory acidosis, we become dependent on our peripheral chemoreceptors to drive ventilation; but they are most sensitive to plasma pO2 levels • Giving a COPD patient pure oxygen?????