Download
1 / 27
270 likes | 451 Views
Self-Measured Blood Pressure Monitoring. Prepared for: Agency for Healthcare Research and Quality (AHRQ) www.ahrq.gov. Outline of Material. Introduction to self-measured blood pressure (SMBP) monitoring Systematic review methods

E N D
Self-Measured Blood Pressure Monitoring Prepared for: Agency for Healthcare Research and Quality (AHRQ) www.ahrq.gov
Outline of Material • Introduction to self-measured blood pressure (SMBP) monitoring • Systematic review methods • The clinical questions addressed by the comparative effectiveness review • Results of studies and evidence-based conclusions about the effectiveness of SMBP in hypertension management, and predictors of SMBP adherence • Gaps in knowledge and future research needs • What to discuss with patients and their caregivers Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
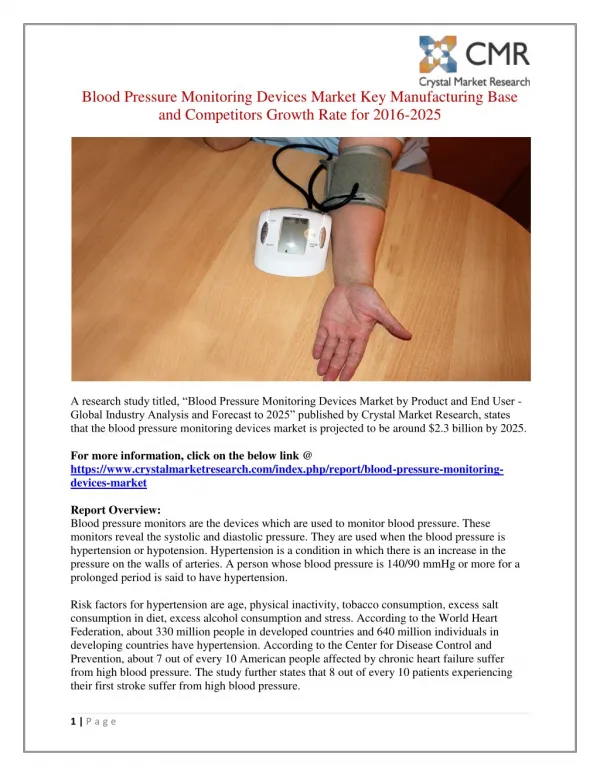
Background: Definition of Hypertension and Its Prevalence • High BP or hypertension is defined as persistently elevated BP 140/90 mmHg in otherwise healthy adults. • The World Health Report 2002estimated that more than 1 billion people have high BP and that 7 million people die from high BP annually. • It is anticipated that the prevalence of BP will continue to rise as the population ages. Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm. Chobanian AV, Bakris GL, Black HR, et al. Hypertension 2003 Dec;42(6):1206-52. PMID: 14656957. World Health Organization. The World Health Report 2002 —Reducing Risks, Promoting Healthy Life. Available at: http://www.who.int/whr/2002/en/.
Background: Disease Burden of Hypertension • Hypertension has been identified as a major risk factor for cardiovascular disease and mortality. • Hypertension is also an important modifiable risk factor for several diseases including: • Coronary artery disease • Stroke • Congestive heart failure • Chronic kidney disease • Peripheral vascular disease Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm. Ezzati M, Oza S, Danaei G, et al. Circulation 2008 Feb 19;117(7):905-14. PMID: 18268146. Chobanian AV, Bakris GL, Black HR, et al. Hypertension 2003 Dec;42(6):1206-52. PMID: 14656957.
Background: Importance of Blood Pressure Control in the Management of Hypertension • Strategies for the management of hypertension involve a combination of antihypertensive medication and lifestyle modifications such as: • Smoking cessation • Moderation of alcohol consumption • Salt restriction and other dietary modifications • Regular exercise • Weight loss in obese persons • Effective BP control has been shown to significantly improve health outcomes and reduce mortality. • A decrease of 5 mmHg in systolic BP is estimated to reduce mortality due to stroke heart disease by 14% and 9% respectively, and all-cause mortality by 7%. Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm. Chobanian AV, Bakris GL, Black HR, et al. Hypertension 2003 Dec;42(6):1206-52. PMID: 14656957.
Background: BP Measurement Strategies — Measurement in the Health Care Setting • For the diagnosis and effective management of hypertension, accurate measurement of BP is crucial. • Strategies for BP measurement include measurement in the health care setting and at home. • Measurement of BP in the clinic or other health care settings has the following limitations: • The need for a period of rest before measurement to obtain reliable readings • The possibility that a patient’s BP may rise as a result of being in the health care setting (termed “white coat” hypertension) • The possibility that a patient’s BP is normal in the clinic, but not outside; (termed “masked” hypertension) Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Background: BP Measurement Strategies — Measurement at Home Background: BP Measurement Strategies — Measurement at Home • There are two BP measurement strategies that can be used at home: • Ambulatory BP monitoring • A noninvasive, fully automated technique in which BP is recorded over an extended period of time. • Requires a technologist to set up and download readings. • Mainly used to diagnose white coat or masked hypertension, or to monitor patients whose BP is hard to control, or is highly variable. • Self-measured BP (SMBP) monitoring • Regular self-measurement of BP by the patient (or a companion). • Readings can be stored and taken to the doctor’s office or transmitted electronically. • Used to detect white coat and masked hypertension, and avoid over-treatment in patients with orthostatic BP changes or hypotensive episodes. • Only SMBP monitoring will be discussed here. Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012 Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Background: SMBP Monitoring Devices • Types of SMBP monitoring devices include: • “Manual”devices — sphygmomanometers that require manual inflation and auscultation • “Semiautomated” devices — manually inflated sphygmomanometers with automated display • “Automated” devices — inflation of sphygmomanometers and BP measurement are both automated • Many devices are commercially available and have been validated by leading organizations. • Patients may require some instruction on device use. Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012 Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm. MedlinePlus Web site. Blood pressure monitors for home. Updated June 10, 2011. Available at: http://www.nlm.nih.gov/medlineplus/ency/article/007482.htm.
Background: Aims of using SMBP Monitoring in the Management of Hypertension • The aims of using SMBP monitoring in hypertension management are: • Avoiding undertreatment of hypertension • Enhancing patient self-participation in disease management • Enhancing adherence to lifestyle and pharmacological interventions • Avoiding overtreatment in patients with lower BP outside the clinic than in it. Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Uncertainties in Existing Biomedical Literature about the role of SMBP Monitoring in Managing Hypertension • It is unclear from existing biomedical literature if SMBP monitoring improves key outcomes related to the management of hypertension including: • BP control • Clinical outcomes • Health care utilization outcomes • It is also uncertain how other support, in addition to SMBP monitoring, affects these key outcomes, when compared with usual care or with SMBP without additional support. • To gain insight into these knowledge gaps, this topic was nominated and developed for comparative effectiveness review with the AHRQ Effective Healthcare Program. Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Agency for Healthcare Research and Quality (AHRQ) Comparative Effectiveness Review (CER) Development • Topics are nominated through a public process, which includes submissions from health care professionals, professional organizations, the private sector, policymakers, members of the public, and others. • A systematic review of all relevant clinical studies is conducted by independent researchers, funded by AHRQ, to synthesize the evidence in a report summarizing what is known and not known about the select clinical issue. The research questions and the results of the report are subject to expert input, peer review, and public comment. • The results of these reviews are summarized into Clinician Research Summaries and Consumer Research Summaries for use in decisionmaking and in discussions with patients. The Summaries and the full report, with references for included and excluded studies, are available at www.effectivehealthcare.ahrq.gov.
Clinical Questions Addressed by the CER (1 of 2) • Key Question (KQ) 1: In people with hypertension (adults and children), does SMBP monitoring, compared to usual care or other interventions without SMBP, have an effect on clinically important outcomes? • How does SMBP monitoring compare to usual care or other interventions without SMBP in its effect on relevant clinical outcomes (cardiovascular events, mortality, patient satisfaction, quality of life, and adverse events related to antihypertensive agents)? • How does SMBP monitoring compare to usual care or other interventions without SMBP in its effect on relevant surrogate outcomes (cardiac measures: left ventricular hypertrophy, left ventricular mass, and left ventricular mass index ) and intermediate outcomes (BP control, BP treatment adherence, or health care process measures)? Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012 Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Clinical Questions Addressed by the CER (2 of 2) • KQ 2: In studies of SMBP monitoring, how do clinical, surrogate, and intermediate outcomes (including SMBP monitoring adherence) vary by the type of additional support provided? • KQ 3: How do different devices for SMBP monitoring compare with each other (specifically semiautomatic or automatic vs. manual) in their effects on clinical, surrogate, and intermediate outcomes (including SMBP monitoring adherence)? • KQ 4: In studies of SMBP monitoring, how does achieving BP control relate to clinical and surrogate outcomes? • KQ 5: How does adherence with SMBP monitoring vary by patient factors? Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No.45. January 2012 Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Rating the Strength of Evidence From the CER • The strength of evidence was classified into four broad categories: Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Comparative Effectiveness of SMBP Monitoring Versus Usual Care (1 of 2) • SMBP improved clinic systolic BP and diastolic BP at 6 months and 12 months when compared with usual care. • SBP net change at 6 months -3.1 mmHg (95% CI ‑5, ‑1.2; P = 0.002) • DBP net change at 6 months -2.0 mmHg (95% CI ‑3.2, ‑0.8; P = 0.001) • SBP net change at 12 months -1.2 mmHg (95% CI ‑3.5, 1.2) • DBP net change at 6 months -0.8 mmHg (95% CI ‑2.5, 1.0) Strength of evidence: moderate Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No.45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Comparative Effectiveness of SMBP Monitoring Versus Usual Care (2 of 2) • Evidence failed to support a difference between SMBP alone versus usual care for the following outcomes: • Quality of life • Number of medications used and medication dosage • Medication adherence • Left ventricular mass index • Patient satisfaction with health care services Strength of evidence: low • Evidence failed to support a difference between SMBP alone versus usual care for health care encounters. Strength of evidence: low Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Comparative Effectiveness of SMBP Monitoring Plus Additional Support Versus Usual Care (1 of 2) • SMBP plus some form of additional support improves BP control when compared with usual care, at least up to 12 months. • The superiority of one form of additional support over another could not be assessed given the heterogeneity in types of additional support used. Strength of evidence: high • Evidence failed to support a difference between SMBP plus additional support versus usual care for the following outcomes: • Quality of life • Number of medications used and medication dosage • Medication adherence • Adverse drug reactions Strength of evidence: low Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Comparative Effectiveness of SMBP Monitoring Plus Additional Support Versus Usual Care (2 of 2) • Evidence failed to support a difference between SMBP plus additional support versus usual care for the number of health care encounters. Strength of evidence: low Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Comparative Effectiveness of SMBP Monitoring With or Without Additional Support (1 of 2) • Evidence fails to support a difference between SMBP with additional support versus SMBP without additional support or with less-intensive additional support for BP control. Strength of evidence: low • Evidence failed to support a difference between SMBP with additional support versus SMBP without additional support or with less-intensive additional support for the following outcomes: • Quality of life • Mental health (anxiety) • Number of medications used and medication dosage • Medication adherence • Adverse drug reactions Strength of evidence: low Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Comparative Effectiveness of SMBP Monitoring With or Without Additional Support (2 of 2) • Evidence failed to support a difference between SMBP with additional support versus SMBP without additional support or with less-intensive additional support for health care encounters. Strength of evidence: low Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No.45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Findings Related to Predictors of SMBP Adherence, Types of SMBP Monitors, and Correlation Between BP Control and Clinical Outcomes • Evidence was insufficient to determine the predictors of SMBP adherence. Strength of evidence: insufficient • Evidence comparing SMBP monitors was insufficient. Strength of evidence: insufficient • Evidence was insufficient to determine how achieving BP control relates to clinical and surrogate outcomes under an SMBP monitoring regime. Strength of evidence: insufficient Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Conclusions (1 of 2) • In the management of hypertension, SMBP alone versus usual care yielded a modest net reduction in in-clinic systolic BP and diastolic BP at 6 months and at 12 months. • Adding clinical support to SMBP led to a consistently greater BP reduction when compared to usual care at up to 12 months of followup. • The evidence was too limited to determine the superiority of any one form of additional clinical support strategy, as modalities varied widely across studies. Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No.45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Conclusions (2 of 2) • The evidence is weak or insufficient to determine if SMBP monitoring with or without additional support has an impact on other outcomes including: • Mortality • Quality of life • Number of medications used and medication dosage • Medication adherence • Health care encounters • Additional research is needed to determine the effect of SMBP monitoring on BP control beyond 12 months and to determine long-term clinical consequences of SMBP monitoring. Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No.45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Knowledge Gaps and Future Research Needs (1 of 3) • The following limitations identified in existing trials should be addressed in future trials: • Short duration of followup (<1 year in most studies) • Heterogeneity in SMBP monitoring and additional support protocols used • Limited evidence on the effect of SMBP monitoring on BP control as a predictor of clinical and surrogate outcomes such as mortality, quality of life, and left ventricular hypertrophy • Lack of studies in children with high BP Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http;//www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Knowledge Gaps and Future Research Needs (2 of 3) • In future studies, SMBP monitoring may be used to characterize a patient’s BP abnormality as uncontrolled or white coat hypertension before trial inclusion to enable appropriate assessment and management. • SMBP monitoring can be burdensome over time. Future studies should help determine the least burdensome protocol(s). • Studies should also be conducted to examine the effects of SMBP monitoring on clinical events. Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No. 45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.
Knowledge Gaps and Future Research Needs (3 of 3) • Other important areas for future research include: • Identifying predictors of adherence to SMBP monitoring. • Approaches for improving adherence to SMBP monitoring. • Improving ways to transmit SMBP results for decisionmaking. • Telemedicine as a means for patient-provider interaction regarding results of SMBP monitoring. • Comparing the ability of SMBP monitoring versus ambulatory BP monitoring to diagnose hypertension.
What To Discuss With Your Patientsand Their Caregivers • The importance of effectively controlling high BP • The link between measuring BP and controlling high BP • The importance of adherence to strategies aimed at managing hypertension such as lifestyle and dietary modifications and medication • How SMBP monitoring allows patients to participate more actively in managing their BP • The types of SMBP devices available and how to operate the device selected for the patient Uhlig K, Balk EM, Patel K, et al. AHRQ Comparative Effectiveness Review No.45. January 2012. Available at: http://www.effectivehealthcare.ahrq.gov/selfmeasuredbp.cfm.