Download
1 / 30
300 likes | 1.27k Views
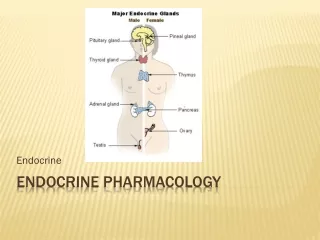
The first 4 slides are from the endocrine pharmacology. Disorders affecting endocrine glands: Deficiency states (more common than excess production) For example if we have a case of hyperthyroidism, we remove the thyroid and end up with a deficiency state then

E N D
Disorders affecting endocrine glands: Deficiency states (more common than excess production) For example if we have a case of hyperthyroidism, we remove the thyroid and end up with a deficiency state then we give the deficient hormone. HRT (hormone replacement therapy)
- Excess production of a specific hormone Inhibitors to the synthetic machinery(which takes time) or Release inhibitors or Specific antagonists
Clinical pharmacology of hormones: - Major clinical use of hormone in the management of deficiency states, the hormone is given in very small amounts HRT ( physiological doses) Supra-physiological doses (pharmacological doses) Hormones are used in diseases not related to the endocrine system, like the use of glucocorticoids in the management of inflammatory conditions, the hormones here are given in larger doses “supra-physiological doses” as compared to those used in HRT. Anti-inflammatory effects (non-endocrine-related diseases)... Use as diagnostic tool (TRH test ....) We use certain hormones in order to see what is the cause of the deficiency.
- The use of some drugs which are not hormones, but used in the management of diseases of endocrine origin Antithyroid drugs(like iodine which is an element), oral hypoglycemic agents… - Some drugs are used to treat diseases not related to the endocrine system but affecting it Anticancerous drugs which affect highly dividing cells→ leading to ♂ & ♀ infertility The use of hormones as contraceptives??? (estrogen, progesterone) they inhibit GnRH axis that will lead to atrophy in the ovaries
Hypothalamus →ADH & Oxytocin → neuro- secretory axons→Posterior pituitary (known as posterior pitutary hormones but they are synthesized in the hypothalamus) • Hypothalamus → Hormones → through a network of capillaries (portal system)→ Anterior pituitary regulating: • ACTH, TSH, LH, FSH ( stimulatory control) • GH, PRL, MSH (stimulatory and inhibitory control)
General characteristics of hypothalamic hormones: TRH, CRH, GHRH, GHIH, GnRH, Dopamine (DA) • Small peptides and polypeptides ( exception DA a.a derivative) of low M.W • Needed in very low concentrations (pg) • Have short t1/2 (natural hormones have very short half life not exceeding 5-10 min) so not given orally or parenterally, synthetic preparations are different. • Act on receptors on plasma membrane
TRH (Protirelin) Tri-peptide, synthetic analogs are available, effective orally and I.V, stimulates TSH synthesis and release, MOA via cAMP, phospholipase C to increase intracellular IP3 Mainly used: • As a diagnostic tool (TRH test) • to assess the function of TSH secreting cells not thyroid • We take blood sample before and after treating the patient with TRH, if the problem is in TRH then it(TRH) can be used for the management of hypothyroidism • Used successfully to treat many cases of hypothyroidism if the anterior pituitary and the thyroid are ok - To treat certain cases of hypothyroidism Dose(don’t worry about them):orally and parenterally.. 50 μg I.V, 5 mg orally, maximum response in 15-30 min, DOA 2-4 hrs
CRH mainly used as diagnostic tool, there are no preparations that could be used in the cases of adrenal insufficiency due to CRH deficiency 41 a.a peptide stimulates synthesis and release of ACTH, stress ↑ CRH release Diagnostic use • GHRH (Hexarelin, Sermorelin) 40 a.a peptide, synthetic given I.V Dignostic use and in the management of certain cases of dwarfism(dwarfism due to hypoythalamic lesion)
GHIH (Somatostatin) (in the control of GH, there is no predominence like in the case of prolactin 14 a.a peptide ↓ secretion of GH, ACTH, TSH, Insulin, Glucagon, Gastrin, Serotonin(could be used in cases of excess production of all these hormones) It is a unique hormone that could be used in the management of excess production of all these hormones It is synthesized in the hypothalamus and in the pancreas Its effects on blood glucose levels are dose dependent( the hormone and its synthetic analogs can cause these effects) Low doses → hypoglycemia (↓ glucagon secretion) High dose → hyperglycemia (↓ insulin secretion)
Octreotide(shorter acting as compared to lanreotide) (given S.C) & Lanreotide (given I.M) Both are given parenterally Synthetic analogs to somatostatin with longer t1/2 (1.5 hrs) mainly used in the management of: • Acromegaly: very severe disease mainly due to adenoma affecting GH secreting cells, fatal in many situations. • Carcinoid syndrome(since it decreases serotonin release from entrochromaffin cells, it’s the drug of choice for carcinoid syndrome • Insulinomas, gastrinomas • Esophageal varices: it stops bleeding in the esophagus • (it has some antiplatelet activity) • ?? Diabetes mellitus since it has an effect on blood glucose level Major side effects: Gall bladder stone formation and platelet abnormalities
Anterior Pituitary Hormonesclassified chemically into: ACTH Simple peptides MSH GH Proteins PRL LH Glycoproteins FSH TSH
For TSH,LH,TSH • (α,β subunits specific gene for α and another one for β transcription, translation α and β proteins glycosylation combination of both to form the complete hormone which is ready for release) all these steps are regulated by the GnRH “hypothalamic hormone” • The α subunit is common between the three hormones, β subunit is responsible for the biological activity (β is different) • HCG hormone also have α and β subunits, its α subunit is also the same, it’s a product of the placenta • Although the β subunit is responsible for the activity, it must be bound to the α subunit for the function to take place.
PosteriorPituitary Hormones Simple peptides (9 a.a) ADH (Vasopressin) Oxytocin • Hypothalamic hormones regulating the anterior pituitary hormones reach the anterior pituitary through a network of capillaries (portal system) whereas ADH and oxytocin reach the posterior pituitary via neurosecretory axons and they are stored in the posterior pitutary.
Anterior Pituitary Hormones in an experiment that was made in animals they found that Hypothalamic lesion or removal → ↓ Ant. Pit H’s except PRL Hypothalamic stimulation → ↑ Ant. Pit H’s except PRL This experiment gives you an idea that prolactin is mainly under inhibition by the hypothalamus (by dopamine) • TSH (binds a specific surface membrane receptor) ↑ T3 & T4 through ↑ cAMP (mainly).. there is a role for the IP3 and Ca but for the exam it is cAMP, also Ca plays a role in exocytosis of the hormone , ↑ Iodine uptake The synthesis includes ↑ iodination and hydrolysis of thyroglobulin ** diagnostic use: mainly used as a diagnostic tool to assess the function of the thyroid gland
ACTH Derived from larger precursor (Pro-opiocortin) ↑ cortisol release and synthesis by the adrenal gland Undergoes circadian rhythm which reflects the circadian rhythm of cortisol (higher during the day, lower during the night for people who sleep at night) And this has clinical significance, whenever we replace or treat patients with cortisol we try as much as possible to limit the physiological pattern of its release this has been shown to be associated with less suppression to the axis particularly if the condition is not related to the axis. Acthar and Cosyntropin (tetracosactrin; Cortrosyn) are synthetic analogs Uses: • Diagnostic use (given I.V or I.M) • Certain cases of adrenal insufficiency (if the adrenal gland is ok)
Growth hormone (Somatropin) HighlySpecies specific: the structure in humans is completely different from that in the cows, pork.. Animal GH cant be used in the management of conditions associated with GH deficiencies in humans MOA Unclear, its effects believed to be mediated through IGFs “insulin like growth factor” (Somatomedins) which are formed in the liver (mainly), kidneys, muscles and other tissues • GH stimulates growth of soft tissues and bones • ↑ lipolysis • ↑ gluconeogenesis & ↓ glucose utilization (diabetogenic effect) • PRL-like activity (and PRL also has some GH-like activity! there is similarity in the structures
Factors ↑ GH release: • Sleep, Arginin, Insulin, Hypoglycemia • β-adrenergic antagonists, Clonidine, Bromocriptine and levodopa in normal individuals • Factors ↓ GH release: • Bromocriptine in acromegalics • Somatostatin synthetic analogs • It is essential to know these factors, because they can be used in deficiency cases or in excess production of growth hormone. • Growth hormone is needed up to a certain age, by the closure of the epiphyseal plate there is no need for growth hormone. Growth hormone deficiency in adults has no clinical significance (doesn’t lead to dwarfism). • That’s why kids are advised to sleep at NIGHT because growth hormone secretion is higher during the night. • Arginin and insulin are sometimes used as provocative tests to assist the function of growth hormone secreting cells, for example sometimes the growth hormone level is on the border and the endocrinologist doesn’t know whether the patient has deficiency or not, so these are used as diagnostic tools. (we give the patient insulin or arginin , if growth hormone increases growth hormone producing cells are functioning) • Bromocriptine and levodopa usually result in paradoxical effect on growth hormone release. • There is similarity in structure between growth hormone and prolactin. • The major and most frequent side effect for insulin therapy is hypoglycemia
Disorders affecting GH secreting cells: • Hypersecretion → if it was before puberty Gigantism if it was after pubertyAcromegaly Rx…Surgery (Management is surgery, but no matter what you do the patient usually dies.); Somatostatin synthetic analogs, DA (dopamine) agonists (Bromocriptine; Cabergoline) and Pegvisomant (GH-receptor antagonist, given SC, major side effects include abnormal liver enzymes and some reports indicated increased growth of GH-secreting pituitary tumors)
Diagnosis is usually easy and obvious, fortunately it is not that common in Jordan (as compared to other diseases like diabetes , rheumatoid arthritis…) • Pegvisomant: is a specific antagonist for growth hormone, but it has sever side effects, to the extent that some people say that some patients died from these side effects rather than the disease itself.
Hyposecretion (common) → Dwarfism Rx… - GH-replacement therapy with S.C or I.M • S.C: subcutaneous preparation,usually given on daily basis. • I.M: intramuscular, given twice or three times per week more convenient • recombinant human GH preparations: Somatropin (Humatrope) Somatrem (Protropin) - Mecasermin (recombinant human IGF-1) or Mecaserminrinfabate (recombinant human IGF-1 + binding protein-3), given SC in dwarf with IGF-1 deficiency not responding to GH, hypoglycemia is a major side effect)
In the past they used growth hormone from humans. • Rule: “whenever you give a hormone you try as much as possible to mimic the exact physiological release of that particular hormone. ” and since the growth hormone is released at night on daily basis, it is better to give the drug as subcutaneous injection at night, until closure of epiphyseal plate. (if the patient is 9 years old he’ll keep taking it until 18) • We can also use IGF-1 in the treatment of dwarfism. Certain types of dwarfism are due to protein mediated effects of growth hormone rather than the defects in the growth hormone secreting cells. Mecasermin is a synthetic recombinant IGF. Mecaserminrinfabate contains binding protein 3 which binds IGF-1, which gives it the advantage of having lower incidence of hypoglycemic attack. HYPOGLYCEMIA is the major side effect to both but it is less frequent with bound IGF.
Side effects of synthetic rHGH products: Water retention, the development of antibodies to HGH, insulin resistance and diabetes, hypertension, carpal tunnel syndrome, abnormal bone growth, reduced life span, disturbed insulin metabolism, leukemia, overgrowth of connective tissue, and tumors, ↑ intracranial pressure with papilledema
Prolactin (PRL) Ant. Pit; Placenta ** Dopamine (DA) ** Has GH-like activity Role in ♂s ??? ↑ PRL (↓ LH & FSH) → ♂ impotency & infertility In ♀s: • Breast development (puberty; pregnancy) • Lactation • ↓ LH & FSH (galactorrhea amenorrhea syndrome)
Prolactin is under the inhibition of dopamine • Prolactin may have a role in the immune system, but its not well understood. • Males have oxytocin but we don’t its role. ( all female hormones are also present in males like prolactin, oxytocin,estrogen, progesterone and females also have testosterone) • Production of prolactin in males is not fully understood except in diseases, because prolactin has been found to inhibit LH,FSH synthesis and release by the pituitary • In some cases of infertilityin males, the sexual function is ok but there is a small increase in prolactin(it doesn’t affect the sexual function but it affects the fertility) • So in both males and females prolactin inhibits Lh & FSH major source of infertility. • In females, its responsible for milk production. Milk ejection is a function of oxytocin. • So at term (after delivery) there is excess production of prolactin that is responsible for milk production and lactation. • Don’t forget this effect of prolactin inhibiting LH,FSH both in males and females • In females its called Galactorrhea-Amenorrhea Syndrome, milk will be produced even in non-pregnant females, there will be some milk production by the breast.
Factors/drugs ↑ PRL: - Pregnancy, sleep, nursing, stress (surgery, exercise) - TRH, Estradiol, DA antagonists (antipsychotics= phenothiazines and haloperidol; metoclopramide..) • Methyldopa, reserpine, diazepam, opiates, meclizine, imipramine… • They will affect fertility • Factors/drugs ↓ PRL: DA agonists ({Bromocriptine: orally effective drug relatively safe drug}, pergolide, levodopa) apomorphine, clonidine , MAO inhibitors (pargyline) Widely used clinically in many situations
Clinical uses to bromocriptine: • Hyperprolactinemia in ♂s and ♀s irrespective of its causes • (increase in prolactin in males: lead to infertility from the male side) • Suppression of lactation(if the lady has a problem and she needs to suppress lactation for example if the baby died in utero, she has to supress lactation because it is a rich media for bacterial growth • Or if she has an infection,usually lactation is stopped after treatment she can breast feed her baby. • Acromegaly (decreases GH release) • Parkinson’s disease (dopamine agonist, crosses the BBB) Bromocriptine is given orally
Good luck Done by: Sarah Qawasmeh LubnaHamdan