Download

1 / 26
950 likes | 6.1k Views
APPLIED ANATOMY OF LUNGS. Dr. G.K. ARAVINDAKSHAN……. 09.01.2012. The respiratory system develops from the ventral wall of the foregut, the sulcus laryngotrachealis during gestation at 3–4 weeks. LRT (lower respiratory tract) arises from laryngotracheal diverticulum .

E N D
APPLIED ANATOMY OF LUNGS Dr. G.K. ARAVINDAKSHAN…… 09.01.2012
The respiratory system develops from the ventral wall of the foregut, the sulcuslaryngotrachealis during gestation at 3–4 weeks. • LRT (lower respiratory tract) arises from laryngotrachealdiverticulum. • Wk 24 – resp bronchi form, respiration is possible • Wk 29 – type II secrete surfactant (reaches adequate levels 2 wks before birth)
The respiratory system develops from the ventral wall of the foregut during gestation at 3–4 weeks (embryonic stage) and continues development during the first 2 years of life and beyond. • The epithelium of the trachea, bronchi, and alveoli originates from the endoderm. • Muscle, cartilage, and connective tissue originate from the mesoderm. • The tracheobronchial tree develops between days 24 and 36 of gestation.
A median bulge develops on the ventral wall of the pharynx at the laryngotracheal groove at days 24–26. • While the laryngotracheal groove is forming, there is a proliferation of the mesenchyme of the primitive mesentery (mediastinum); from this mesenchyme, the cartilage, muscle, and connective tissue of the lungs will develop. • By the 28th day, the bulge has formed into the right and left lung buds. • As the lung buds elongate, lateral invagination of the mesoderm constitutes the tracheoesophageal septum, which separates the esophagus and trachea
The separation of alimentary and respiratory structures is not always completed successfully. • Defective or incomplete separation is one of the most frequent congenital anomalies. • At 28–30 days, the lung buds continue to elongate, forming the primary bronchi, which develop monopodial outgrowths that lengthen into the segmental bronchi. • At the same time, the tissue vascular supply shifts from the splenic plexus to the definite pulmonary arteries
The right lung grows faster than the left, being both larger and having more generations of bronchial branching. At approximately 10 weeks, cartilage appears in the trachea and primary bronchi and at 16 weeks in the segmental bronchi. • At 24 weeks, during the “alveolar stage,” the distal ends of the ducts open and the alveoli are formed.
After 24 weeks, there is an apparent decrease in the number of generations of bronchi due to epithelial changes in terminal bronchioles and their conversion into respiratory bronchioles. • Alveoli first appear at approximately 32 weeks gestation and are usually present by 36 weeks. Alveoli continue to multiply until 300 million have formed. This number is reached when the child is about 8 years old.
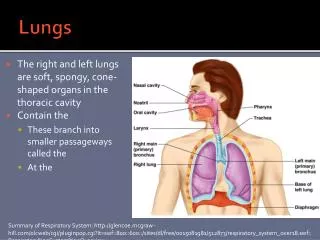
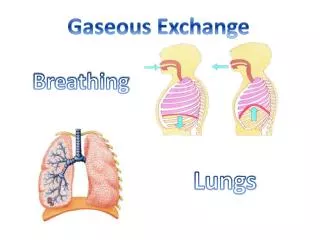
During life the lungs are soft & spongy and very elastic. • At childhood age the lungs are pinkish, but with the inhalation of dust particles they became dark. • Each lung is conical in shape, covered with visceral pleura, & suspended free in its own pleural cavity, being attached to the mediastinum only by its root.
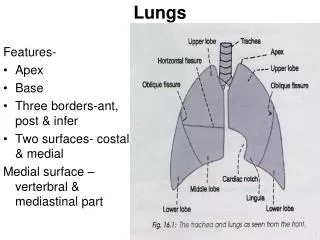
Each lung has a blunt apex, concave base, convex costal surface, concave mediastinal surface, hilum in middle surface, cardiac notch in left lung. • Regarding lobes & fissures it is divided by oblique & horizontal fissure: the upper, middle & lower lobes.
Broncholumonary segments are the surical units of lungs. • Each bronchus passes to a structurally & functionally dependent unit of a lung lobe called a BRONCHOPULOMNARY SEGMENT… surrounded by connective tissue.
The lungs • The apex of the lung closely follows the line of the cervical pleura and the surface marking of the anterior border of the right lung corresponds to that of the right mediastinal pleura. • On the left side, however, the anterior border has a distinct notch (the cardiac notch) which passes behind the 5th and 6th costal cartilages.
The lower border of the lung has an excursion of as much as 2–3in (5–8cm) in the extremes of respiration, but in the neutral position (midway between inspiration and expiration) it lies along a line which crosses the 6th rib in the midclavicular line, the 8th rib in the midaxillary line, and reaches the 10th rib adjacent to the vertebral column posteriorly.
The oblique fissure, which divides the lung into upper and lower lobes, is indicated on the surface by a line drawn obliquely downwards and outwards from 1in (2.5cm) lateral to the spine of the 5th thoracic vertebra to the 6th costal cartilage about 1.5in (4cm) from the midline. • The line of the oblique fissure then corresponds to the position of the medial border of the scapula.
The surface markings of the transverse fissure (separating the middle and upper lobes of the right lung) is a line drawn horizontally along the 4th costal cartilage and meeting the oblique fissure where the latter crosses the 5thrib.
Clinical Anatomy of Lung • Usually, the infectn of a segment remains restricted to it, although some infections like TB, may spread one segment to another. resection of a bronchopulmonaryseg. removal of one lobe- Lobectomy removal of whole lung - Pneumonectomy
Tumour of upper lobe of lung causes certain press. Effects -venous engorgement & oedema of face & upper limb -Diminished pulse -Paralysis of the cupola -Hoarseness of voice etc.
Breath sounds from the upper lobe are best heard in front & those from the lower lobe best heard on the back. • The middle lobe does not reach the chest wall behind & auscultated in front b/n 4th and 6th ribs. • Breath sounds from all lobes are heard along the mid-axillary line. • Accidental injury.
Ds.s, such as silicosis, asbestosis, cancer and pneumonia interfere with the process of expanding the lung in inspiration. • Environmental lung diseases.
bronchi • Aspiration of foreign bodies. • Widening & distortion of the angle between the bronchi.