Download
1 / 18
180 likes | 337 Views
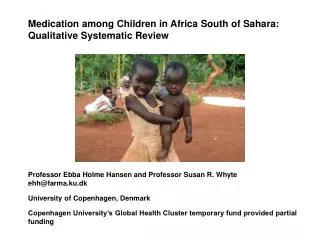
Emotional well-being among orphaned and vulnerable children in two communities in South Africa. Simbayi L, Setswe G , Jooste S, Davids A & Tabane C ICP 2012 Conference 25 July 2012. Background (1).

E N D
Emotional well-being among orphaned and vulnerable children in two communities in South Africa Simbayi L, Setswe G, Jooste S, Davids A & Tabane C ICP 2012 Conference 25 July 2012
Background (1) • The HSRC and its partners were funded by the WK Kellogg Foundation (WKKF) to develop and implement a 5-year intervention project for OVC in SA, Botswana and Zimbabwe. • Nelson Mandela Children's Fund (NMCF) worked with CBOs to support implementation of OVC interventions in South Africa. • The aim of the project was to empower the communities in selected communities to develop best practice interventions for OVC. • This part of the project was to evaluate emotional well-being of OVC in two communities in South Africa
Research & Intervention sites • The study was conducted in Kanana Township in North West province and Kopanong Municipality in the Free State province. • Kanana is a township near the town of Orkney in Dr Kenneth Kaunda District Municipality which had a population of 66,936 in 19,702 householdsin 2001 covering an area of 9.90 km2 . • Kopanong comprises 8 towns in southern FS: Reddersburg, Smithfield, Bethulie, Jagersfontein, Philippolis, Springfontein, Reddersburg, Fauresmith with a population less than 56,000 in 2001. Kanana Free State Province Kopanong Sources: Census 2001. http://census.adrianfrith.com/place/61909. http://www.sa-venues.com/maps/north-west-regional.htm
Method • Study Design: Cross-sectional surveys were conducted at the two sites • Population: Parents/guardians of OVC and children aged 6-14 and 15-18 years at both sites • Sampling: a stratified sampling approach: • Parents/Guardians of OVC n = 1,036were stratified into: • Parents/Guardians of OVC aged 6-14 • Parents/Guardians of OVC aged 15-18
Demographics: Parents/Guardians of OVC (n = 1036) • A substantial proportion (51.9%) of the children were taken into care because one or both of their parents had died. • Grandparents (20.8%), in particular maternal grandparents serving as caregivers for the OVC raised some concerns in terms of sustainability of care, and the heavy reliance of affected families on government pension grants (13.3%).
Demographics: Parents/Guardians of OVC • A fifth (20.9%) of the parents/guardians had had no formal schooling. • Full or part-time employment was low (22.2%), as was self-employment (17.4%). • A third reported looking for work (34.3%), while a small percentage reported being too sick to work (5.3%). • The majority (96.6%) reported knowing about HIV/AIDS and cited poverty and HIV/AIDS as being the major reasons for orphanhood in the area. • Approximately half the number of guardians mentioned that they do talk to their children about sex (51.3%), HIV/AIDS (59%) and reproductive health (50.4%).
Needs of OVC (n = 1036) • The three most commonly cited needs of OVC were: • food (88.4%), • financial support (83.1%), • educational support (71.1%). • Only 21.4% identified socio-emotional support as a need for OVC. • Most guardians (97.3%) said that their own children reacted positively to the addition of this child to the household.
Demographics: Children aged 6-14 (n = 859) • Nearly one third (30%) were orphans • 24% were paternal orphans • 17% maternal orphans, and • 3% double orphans. • One fifth (17%) did not know the whereabouts of their fathers • Few (1.3%) were heads of households. • 81.3% of the children were happy with their guardian. • The majority (92%) belonged to a faith group.
Emotional wellbeing: Children aged 6-14 (n = 859) • Only 16.4% of the respondents inherited the house they lived in before their parent/s died. • Only 11% of the respondents concerned were consulted in the distribution of family goods. • A sizable minority (42.1%) had special personal items such as photos and other things that belonged to their deceased parents.
Emotional wellbeing: Children aged 6-14 • A large group (43.5%) of the children reported that they often and sometimes had trouble sleeping. • On the other hand, the number of children feeling happy sometimes or often(91%), is encouraging for it suggests proper caring and love by the current caregivers. • Those older enough to envision the future wished for a good profession (30.7%) and education (17.3%).
Demographics: Children aged 15-18 (n = 496) • Nearly one third (36%) were orphans • 36% were paternal orphans • 27% were maternal orphans • 8% double orphans • A quarter 25% did not know if their fathers were dead or alive • Nineteen (3.8%) were heads of households, 14 males and five females. • An overwhelming majority of children (95.4%) believed their parents/guardians should discuss their health condition to prepare them emotionally for their long illness and death. • 53.1% of orphans lived in the same house as they did prior to their parents death.
Emotional wellbeing: Children aged 15-18 • Many children (68.2%) were sad when they were separated from their siblings and other children known to them. • Just over a third (38.3%) of the OVC stated that they would like their guardians to give them more financial support or food or clothing. • Nonmaterial support (more emotional support and improved communication was mentioned by children (13.5%).
Emotional wellbeing: Children aged 15-18 • The overwhelming majority (90.7%) were very staunch members of their religious groups. • A quarter of orphans (24.8%) reported being still bothered by their parent(s) or guardian(s) death. • Over half of children (55%) sometimes/often felt like crying. • Some 9.2% reported sometimes/often felt like killing themselves, nearly one fifth (19.4%) of those felt like doing so in the 2 weeks prior to the interview.
Emotional wellbeing: Children aged 15-18 • A majority indicated that they were: • Unhappy at times (77%) • Very angry (73%) • Avoided places or things (65%) • Had scary dreams or nightmares (57%) • Had panic attacks (57%) • A majority (74.4%) of them felt hopeful about the future especially education.
Recommendations (1) • Interventions should begin during the guardian’s illness. Prepare parents and guardians to deal with their illness, and include emotional and practical issues (writing a will and leaving instructions on their children’s future welfare). • Material supportis a second support tier as young children need the stability of a daily routine of physical containment and nurturance. • Legal supportfor children not to lose their inheritance and assets is critical.
Recommendations (2) • Micro-financeprogrammes should target poor communities and OVC caregivers. • Home-based carersneed training in emotional and child development issues, the impact of a terminal illness on children’s psyche to assist households to cope with their situation. • Religious institutionshave an important role to play in the protection of children given high levels of religiosity.
Recommendations (3) • Male role modelsshould be used in training, counseling, mentoring and related programs to make up for the glaring absent father gap in the lives of OVC. • NGOs, CBOs and FBOsare central partners to government initiatives to implement its programmes in communities and should be a key means of facilitating transfer of resources to local communities.
Acknowledgements • WK Kellogg Foundation • Human Sciences Research Council (HSRC) • Nelson Mandela Children’s Fund (NMCF) • DiketsoEsengDipuo (DEDI) CBO in Kopanong • Child Welfare North West in Kanana and KOSH area 18