Download
1 / 9
90 likes | 249 Views
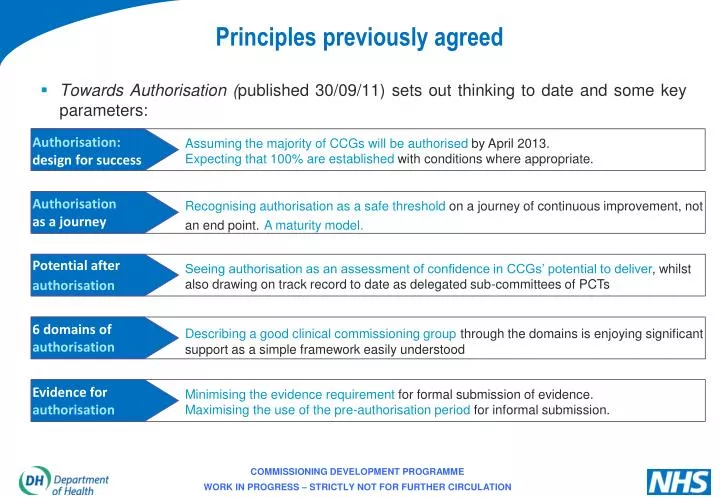
Principles previously agreed. Towards Authorisation ( published 30/09/11) sets out thinking to date and some key parameters:. Authorisation: design for success.

E N D
Principles previously agreed Towards Authorisation (published 30/09/11) sets out thinking to date and some key parameters: Authorisation:design for success Assuming the majority of CCGs will be authorised by April 2013.Expecting that 100% are established with conditions where appropriate. Authorisationas a journey Recognising authorisation as a safe threshold on ajourney of continuous improvement, not an end point.A maturity model. Potential after authorisation Seeing authorisation as an assessment of confidence in CCGs’ potential to deliver, whilst also drawing on track record to date as delegated sub-committees of PCTs 6 domains of authorisation Describing a good clinical commissioning groupthrough the domains is enjoying significant support as a simple framework easily understood Evidence for authorisation Minimising the evidence requirement for formal submission of evidence.Maximisingthe use of the pre-authorisation period for informal submission.
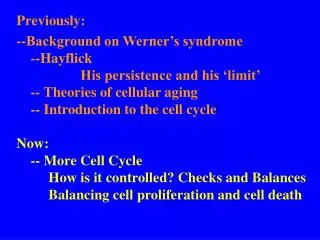
1 2 6 A strong clinical and multi-professional focus which brings real added value Meaningful engagement with patients, carers and their communities Great leaders who individually and collectively can make a real difference Clear and credible plans which continue to deliver the QIPP challenge within financial resources, in line with national requirements (including outcomes) and local joint health and wellbeing strategies 3 4 Proper constitutional and governance arrangements, with the capacity and capability to deliver all their duties and responsibilities, including financial control, as well as effectively commission all the services for which they are responsible 5 Collaborative arrangements for commissioning with other clinical commissioning groups, local authorities and the NHS Commissioning Board as well as the appropriate external commissioning support Authorisation remains based on six domains as widely discussed
Authorisation content: a clear line of sight Evidence for authorisation Threshold for authorisation Criteria Potential beyond authorisation
Draft application submission list • Authorisation application form • CCG constitution and other documents detailing governance arrangements (please specify) • CCG Organogram • Case studies (please specify) • Draft Joint Strategic Needs Assessment • Financial management arrangements compliant with national requirements • Health and Wellbeing Board minutes and reports • Joint Health and Wellbeing Strategy • Letter of support for CCG Chair • List of collaborative and joint commissioning arrangements • Minutes of multi-professional meetings • Organisational Development Plan • SLA or MoU with assured commissioning support provider • 2012-13 contracts • 2012-13 Integrated Plan and draft commissioning intentions for 2013-14 • 360° stakeholder survey report and CCG comment
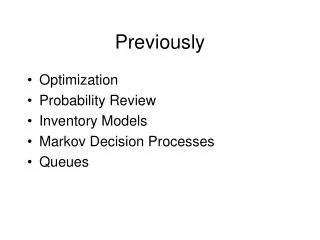
Pre-application Application NHSCB assessment • Covering: • Most aspects of governance • Organisational form • Commissioning support arrangements Enabling the CCG to set out factual details relevant to its application, but also to demonstrate compliance / self-certify against a number of authorisation criteria • Covering all aspects of authorisation • Desktop review • 360 review • Site visit Phases of Authorisation
CCG performance and population health profiles • Provided to all CCGs at least one month before the application date for their wave, profiles will provide the following data configured at CCG level: • Geography - including the relationship between the CCG and their Local Authority, and the relationship between a CCG’s registered and resident population; • Demographic and socioeconomic profile - e.g. age/ sex/ Index of Multiple Deprivation; • Population level outcomes data - e.g. QOF; • Activity and outcomes data (e.g. the latter from inpatient survey) split by main provider; • Performance data; • Finance - including baselines, fairshares and risk of overspend given the CCG populations. • CCG profiles will be used by the assessor team to understand the challenges facing applicant CCGs and will form part of the data triangulation on track record, planning, prioritisation and financial management.
360° Stakeholder Review Objective Objective The survey will assess whether CCGs have been developing strong foundations for successful relationships with all key stakeholders and examine the potential for these relationships to evolve. The survey will assess whether CCGs have been developing strong foundations for successful relationships with all key stakeholders and examine the potential for these relationships to evolve Participants c40-45 stakeholders per CCG to include GP constituent practices, other CCGs, (shadow) Heath & Wellbeing boards, Local Authorities, LINks/(shadow) Healthwatch, NHS providers… c40-45 stakeholders per CCG to include GP constituent practices, other CCGs, (shadow) Heath & Wellbeing boards, Local Authorities, LINks/(shadow) Healthwatch, NHS providers… Timing CCGs to provide participants’ contact details approx. 8 weeks prior to authorisation. Survey results will be returned to CCGs just prior to authorisation leaving enough time for their comment Format An online survey that will include generic questions to all participants plus small banks of stakeholder-specific questions. Total survey length will be approx. 15-20 mins Content Will cover themes such as stakeholders’ experiences of working with emerging CCGs so far and their opinions of CCGs’ potential to deliver quality, clinically-led commissioning in the future Role of CCGs To provide accurate stakeholder contact in a timely manner and to submit the survey results plus CCG comments as part of the authorisation documentation Assistance provided Information materials and a website will help inform CCGs and their stakeholders as to the survey’s purpose and content. A dedicated email and enquiry line will also be made available Non-response Non-respondents will be followed up with reminder emails and a phone call. Any stakeholders not wishing to participate in the full survey will be asked to complete a non-response survey
Case Studies • CCGs are asked to submit case studies as part of their application, and they will also be used to establish a national library of best practice emerging from clinical commissioning • They are an opportunity for CCGs to demonstrate their ability to deliver improvements (e.g. in access to services, health outcomes, service quality/productivity, reducing health inequalities) across all six domains. They also form part of the core evidence for authorisation in the following areas: • Member practice involvement in decision-making • Taking devolved responsibility for specific commissioning budgets/areas/programmes from local PCT cluster • Innovation - e.g. through use of intelligence/information, service redesign, through collaboration with other clinicians, engagement with the public and patients, use of technology • Leadership and leadership development • Enhanced clinical involvement in service redesign and improvement • Involvement in 2012-13 contracting round • Measurable improvements in productivity and quality delivered – e.g. improved holistic management of patients with chronic conditions and those at end of life • Engaging different groups and communities through a range of communications channels in the development of vision, commissioning plan, or in broader CCG decision-making processes • CCG collaboration with other CCGs and a multi-disciplinary range of clinicians