Download

1 / 86
980 likes | 1.13k Views
Arterial Hypertension. Presented By: Dr Emami. hypertension is the most common reason for office visits of non-pregnant adults to physicians in the United States and for use of prescription drugs.

E N D
Arterial Hypertension Presented By: Dr Emami
hypertension is the most common reason for office visits of non-pregnant adults to physicians in the United States and for use of prescription drugs.
Despite the prevalence of hypertension and its associated complications, control of the disease is far from adequate . Data from NHANES show that only 45 percent of persons with hypertension have their blood pressure under control, defined as a level below 140/90 mmHg
DEFINITIONS Hypertension was defined as a blood pressure ≥140/90 mmHg Normal BP: systolic <120 mmHg and diastolic <80 Prehypertension: systolic 120-139 mmHg or diastolic 80-89 Hypertension: Stage 1: systolic 140-159 mmHg or diastolic 90-99 mmHg Stage 2: systolic ≥160 or diastolic ≥100 mmHg
Isolated systolic hypertension isolated diastolic hypertension These definitions apply to adults on no antihypertensive medications and who are not acutely ill. If there is a disparity in category between the systolic and diastolic pressures, the higher value determines the severity of the hypertension.
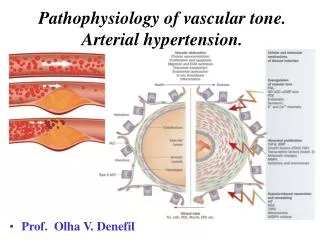
ESSENTIAL (PRIMARY) HYPERTENSION Pathogenesis — is poorly understood. ; Increased sympathetic neural activity, with enhanced beta-adrenergic responsiveness. Increased angiotensin II activity and mineralocorticoid excess. Hypertension is about twice as common in subjects who have one or two hypertensive parents genetic factors account for approximately 30 percent of the variation in blood pressure in various populations Reduced adult nephron mass may predispose to hypertension, which may be related to genetic factors, intrauterine developmental disturbance (eg, hypoxia, drugs, nutritional deficiency)
Risk factors: • Race • salt intake :increased salt intake is a necessary but not sufficient cause for hypertension. • excess alcohol intake • Obesity is associated with an increased prevalence and incidence of hypertension • Physical inactivity • Dyslipidemia : may also be associated with the development of hypertension, and is independent of obesity
COMPLICATIONS —The likelihood of developing the complications varies with the blood pressure. The increase in risk begins as the blood pressure rises above 110/75 mmHg in all age groups. In older patients, systolic pressure and perhaps pulse pressure are more powerful determinants of risk than diastolic pressure .
Screening The optimal interval for screening for hypertension is not known. guidelines on screening for high blood pressure recommend screening every two years for persons with systolic and diastolic pressures below 120 mmHg and 80 mmHg, respectively and yearly for persons with a systolic pressure of 120 to 139 mmHg or a diastolic pressure of 80 to 89 mmHg
DX In the absence of end-organ damage, the diagnosis of mild hypertension should not be made until the blood pressure has been measured on at least three to six visits, spaced over a period of weeks to months. the blood pressure drops by an average of 10 to 15 mmHg between visits one and three in patients who appear to have mild hypertension on a first visit to a new doctor, with a stable value not being achieved until more than six visits in some cases Thus, many patients considered to be hypertensive at the initial visit are in fact normotensive.
Technique of blood pressure measurement in the diagnosis of hypertension
Correct measurement and interpretation of the blood pressure is essential in the diagnosis and management of hypertension. Proper BP machine calibration, training of personnel, positioning of patient, and selection of cuff size are all essential.
TIME OF MEASUREMENT— For the diagnosis of hypertension, multiple readings should be taken at various times. Extraneous variables that can influence the BP should be avoided in the 60 minutes prior to evaluation. These include food intake, strenuous exercise ,smoking, and the ingestion of caffeine. Smoking transiently raises the BP; thus, the office BP may underestimatethe usual BP in a heavy smoker who has not smoked for more than 30 minutes before the measurement is made. Caffeine intake can raise the BP acutely, Taking the BP in a cool room (12ºC or 54ºF) or while the patient is talking can raise the measured value by as much as 8 to 15 mmHg.
TYPE OF MEASUREMENT DEVICE Mercury sphygmomanometers provide the most accurate measurement of BP. Aneroid sphygmomanometers, which are used in many offices, should be checked against a mercury device since the air gauge may be in error. Automated oscillometric BP measuring devices are increasingly being used in medical offices, and for home monitoring. The readings are typically lower than BP obtained with the auscultatory method.. The disadvantages are that the oscillometric method has somewhat greater inherent error and epidemiologic data are based on auscultatory methods. advantages are that observer error and training are minimal.
CUFF SIZE— Use of a proper-sized cuff is essential. If too small a cuff is used, can lead to overestimation of the systolic pressure by as much as 10 to 50 mmHg in obese patients. The length of the BP cuff bladder should be 80 percent, and the width at least 40 percent of the circumference of the upper arm. This width recommendation cannot be practically maintained in obese patients.
PATIENT POSITION — The BP is ideally taken in the sitting position with the back supported Supine values tend to be slightly different, Supine and standing measurements should always be taken in the elderly to detect postural hypotension The arm should be supported at the level of the heart. The mercury manometer should be visible but does not have to be at the level of the heart The patient should sit quietly for five minutes before the BP is measured . Even under optimal conditions, many patients are apprehensive when seeing the physician, resulting in an acute rise in BP.
CUFF PLACEMENT — The blood pressure cuff should be placed with the bladder midline over the brachial artery pulsation, with the arm without restrictive clothing (the patient's sleeve should not be rolled up as this may act as a tourniquet) If possible, the lower end of the blood pressure cuff should be two to three centimeters above the antecubitalfossato minimize artifactual noise related to the stethoscope touching the cuff.
TECHNIQUE OF MEASUREMENT— The cuff should be inflated to a pressure approximately 30 mmHg greater than systolic, as estimated from the disappearance of the pulse in the brachial artery by palpation The auscultatory gap is associated with increased arterial stiffness and carotid atherosclerosis; it may therefore identify patients at increased risk of cardiovascular disease Once the cuff is adequately placed and inflated, the following steps should be followed;
Neither the patient nor the observer should talk during the measurement The BP should be taken with the patient's arm supported at the level of the heart. The mercury manometer should be visible but does not have to be at the level of the heart The stethoscope should be placed lightly over the brachial artery, since the use of excessive pressure can increase turbulence and delay the disappearance of sound. The net effect is that the diastolic pressure reading may be artifactually reduced by up to 10 to 15 mmHg The cuff should be deflated slowly at a rate of 2 to 3 mmHg per heartbeat
The systolic pressure is equal to the pressure at which the brachial pulse can first be palpated . or the pressure at which the pulse is first heard by auscultation (Korotkoff phase I). As the cuff is deflated below the systolic pressure, the pulse continues to be heard until there is abrupt muffling (phase IV) and, approximately 8 to 10 mmHg later, disappearance of sound (phase V) The diastolic pressure is generally equal to phase V
the point of muffling should be used in those patients in whom there is more than a 10 mmHg difference between phases IV and V This can occur in children, and in high-output states such as thyrotoxicosis, anemia, and aortic regurgitation.
The BP should be measured initially in both arms.If there is a disparity due to a unilateral arterial lesion, the arm with higher pressure should be used. The BP should be taken at least twice on each visit, with the measurements separated by one to two minutes to allow the release of trapped blood. If the second value is more than 5 mmHg different from the first, continued measurements should be made until a stable value is attained.
Leg blood pressure — There are occasional patients in whom the blood pressure needs to be measured in the legs. The classic example is with suspected coarctation of the aorta in which there is an arm-to-leg gradient. Blood pressure should be taken in the leg among women with breast cancer who have undergone bilateral axillary lymph node dissection, If there has been unilateral axillary node dissection, it is recommended that the BP should always be taken in the contralateral arm.
The principles of blood pressure measurement in the leg are similar to the arm. An appropriate-sized thigh cuff is essential. The systolic pressure in the leg in normal subjects is usually 10 to 20 percent higher than that in the brachial artery.
Wrist blood pressure — may be more practical in obese people, since wrist diameter is not significantly affected. Systolic BP rises, and diastolic BP falls, in more distal arteries. In the wrist, the hydrostatic pressure related to the lower position of the wrist relative to the heart can result in a further false elevation of BP. This can be minimized by taking the BP with the wrist kept at the level of the heart.
MULTIPLE BLOOD PRESSURE MEASUREMENTS in the absence of end-organ damage, the diagnosis of mild hypertension should not be made until the blood pressure has been measured on at least two additional visits, spaced over a period of one week or more . Sequential studies have shown that the BP drops by an average of 10 to 15 mmHg between the first and third visits in newly diagnosed patients with a stable value not being achieved until more than six visits in some cases Thus, many patients considered to be hypertensive at the initial visit are in fact normal.
in patients diagnosed as being hypertensive on a first visit to a new physician, there is a mean 15 and 7 mmHg fall in the systolic and diastolic BP, respectively, by the third visitwith some patients not reaching a stable value until the sixth visit Thus, it has been recommended that a patient with mild to moderate elevation in BP should not be diagnosed with hypertension unless the BP remains elevated after three to six visits, unlessthere is evidence of ongoing end-organ damage. the prevalence of white coat hypertension ranges from 10 to more than 20 percent, and appears to be higher in children and the elderly
White coat hypertension can also be seen in patients with apparently resistant hypertension The likelihood of normal ambulatory pressures is low (less than 5 percent) in patients with office diastolic pressures ≥105 mmHg but such patients may still have a white coat effect underestimates the efficacy of therapy
the optimal approach to patients with white coat hypertension is uncertain. If therapy is withheld because of a normal ambulatory BP, careful monitoring is still indicated for the possible development of worsening hypertension or of end-organ damage, while the patient is encouraged to modify unhealthy lifestyle habits.
INTERPRETATION OF ABPM — One of the unresolved issues in ambulatory monitoring is the definition of what constitutes normal and elevated blood pressure Most experts agree that 24 hour blood pressure <130/80 mmHg is probably normal, and ≥135/85 mmHg is probably abnormal A daytime ambulatory average BP below 135/85 is normotension.
INDICATIONS FOR ABPM • Suspected white coat hypertension • Suspected episodic hypertension (eg,pheo) • Hypertension resistant to increasing medications • symptoms while taking antihypertensive medications • Autonomic dysfunction • To establish nondipper status or nocturnal hypertension • Large variations in self-measured blood pressure values
PROGNOSTIC VALUE OF ABPM Prediction of cardiovascular risk — the risk of hypertensive cardiovascular complications (including both the development and regression of LVH with treatment) correlates more closely with 24-hour or daytime ABPM than with the office pressure However, the difference in prognostic accuracy between ABPM and office readings might be diminished by obtaining repeated BP measurements during the same visit, or by measuring BP in a standardized fashion with appropriate equipment
Normal Pattern • The usual fall in BP at night is largely the result of sleep and inactivity rather than the time of day • Whereas the nocturnal fall averages approximately 15% in those who are active during the day, it is only about 5%in those who remain in bed for the entire 24 hours • The usual falls in BP and heart rate that occur with sleep reflect a decrease in sympathetic nervous tone. • In healthy young men, plasma catecholamine levels fell during rapid-eye-movement sleep, whereas awakening immediately increased epinephrine, and subsequent standing induced a marked increase in norepinephrine
:Associations with Nondipping • Older age (Staessen et al., 1997) • Cognitive dysfunction (Van Boxtel et al., 1998) • Diabetes (Björklund et al., 2002) • Obesity (Kotsis et al., 2005) • African Americans (Jehn et al., 2008) and Hispanics (Hyman et al., 2000) • Impaired endothelium-dependent vasodilation (Higashi et al., 2002) • Elevated levels of markers of cellular adhesion and inflammation (Von Känel et al., 2004) • Left ventricular hypertrophy (Cuspidi et al., 2004) • Intracranial hemorrhage (Tsivgoulis et al., 2005) • Loss of renal function (Fukuda et al., 2004) • Mortality from cardiovascular disease (Redon & Lurbe, 2008)
Nocturnal blood pressure and nondippers The average nocturnal BP is approximately 15 percent lower than daytime values in both normals and hypertensive patients Failure of the BP to fall by at least 10 percent during sleep is called nondipping. Independent of the degree of hypertension, nondipping is a risk factor for the development of LVH as well as HF and other cardiovascular complications Nondipping has also been associated with microalbuminuriaand faster progression of nephropathy in patients with diabetes mellitus. nondipping may be a risk factor for decline in GFR, and ESRD and death among patients with CKD
HOME BP MEASUREMENTS In view of the cost and limited availability of ambulatory monitoring, increasing attention is being given to home Such self-recorded casual BP measurements taken at home or daytime or work correlate more closely with the results of 24-hour ambulatory monitoring than with the BP taken in the office. home BP measurements may be more predictive of adverse outcomes (eg, stroke, end-stage renal disease) than clinic blood pressures patient self-monitoring of BP at home may improve BP control, especially if combined with behavioral interventions
HBPM should become a routine component of BP measurement in the majority of patients with known or suspected hypertension.
Two to three readings should be taken while the subject is resting in the seated position, both in the morning and at night, over a period of 1 W . • A total of ≥12 readings are recommended for making clinical decisions. • The target HBPM goal for treatment is less than 135/85 mm Hg
Use a 7-day measurement period with two to three measurements each morning and two to three measurements in the evening at prestipulated times (an average of 12 morning and 12 evening measurements). • Exclude the first-day measurements from the analyses to remove the alerting reaction.
It is recommended that the BP should be regularly measured (by either the patient or other person) at work and at home In addition to improved control of the BP, potential advantages of home BP monitoring include identification of white coat hypertension, assessment of the response to antihypertensive medications, and improvement in patient compliance.
The potential problems with outpatient BP measurements can be minimized by providing adequate training, and periodically checking the machine for accuracy . As with ambulatory monitoring, the BP taken by the patient varies widely during the day, being influenced by factors such as stress (particularly at work), smoking, caffeine intake, natural circadian variation, and exercise . Thus, multiple readings should be taken to determine the average level.
The timing of antihypertensive medications must also be considered. With short-acting drugs (eg, captopril, atenolol), the BP may fall to normal or even below normal one to two hours after therapy and then gradually increase to elevated levels until the next dose is taken. This problem can be minimized by having the outpatient BP measured 30 to 60 minutes before taking medications, preferably in the early morning to assess for possible inadequate overnight BP control.
the BP should be measured at roughly the same time each day and the relation to meals and medications noted. The patient should be instructed to wait to measure the BP if they have recently eaten a meal or exercised.
Cuff inflation hypertension — A possible problem with self-measurement of BP is that the muscular activity used to inflate the cuff can acutely raise the BP by as much as 12/9 mmHg, an effect called cuff inflation hypertension that dissipates within 5 to 20 seconds (average 7 seconds . ) Thus, inflating the cuff to at least 30 mmHg above systolic and then allowing the sphygmomanometer to fall no more than 2 to 3 mmHg per heartbeat is desirable both for accurate measurement and to permit this exertional effect to disappear