Download
1 / 28
280 likes | 479 Views
2007 Guidelines for the Management of Arterial Hypertension. dr Toni Badia UO Cardiologia Ospedale di Prato. Category. Systolic. Diastolic. Optimal. <120. and. <80. Normal. 120-129. and/or. 80-84. High Normal. 130-139. and/or. 85-89. Grade 1 Hype rtension. 140-159. and/or.

E N D
2007 Guidelines for the Management of Arterial Hypertension dr Toni BadiaUO CardiologiaOspedale di Prato
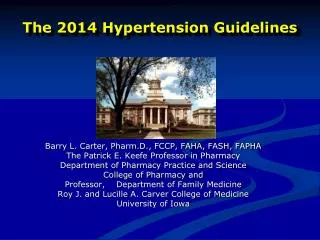
Category Systolic Diastolic Optimal <120 and <80 Normal 120-129 and/or 80-84 High Normal 130-139 and/or 85-89 Grade 1 Hypertension 140-159 and/or 90-99 Grade 2 Hypertension 160-179 and/or 100-109 Isolated Systolic Hypertension ≥140 and <90 Definitions and Classification of Blood Pressure Levels (mmHg) Grade 3 Hypertension ≥180 and/or ≥110
Blood Pressure Thresholds (mmHg) forDefinition of Hypertension with Different Types of Measurement
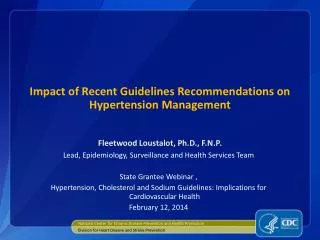
Stratification of CV risk in four categories Blood pressure (mmHg) SBP: systolic blood pressure; DBP: diastolic blood pressure; CV: cardiovascular; HT: hypertension. Low, moderate, high, very high risa refer to 10year risk of a CV fatal or non-fatal event. The term “added” indicates that in all categories risk is greater than average. OD: subclinical organ damage; MS: metabolic syndrome.
Stratification of CV risk in four categories Blood pressure (mmHg) SBP: systolic blood pressure; DBP: diastolic blood pressure; CV: cardiovascular; HT: hypertension. Low, moderate, high, very high risa refer to 10year risk of a CV fatal or non-fatal event. The term “added” indicates that in all categories risk is greater than average. OD: subclinical organ damage; MS: metabolic syndrome.
Secondary hypertension • Severe blood pressure elevation • Sudden onset or worsening • Blood pressure responding poorly to drug therapy
Laboratory Investigations Routine investigations • Urine strip test for protein and blood (complemented by microalbuminuria dipstick test and microscopic examination) • Serum creatinine and electrolytes • Estimated creatinine clearance (Cockroft-Gault formula) • Blood glucose - ideally fasted • Blood lipid profile (at least total and high density lipoprotein (HDL) cholesterol) – ideally fasted for consideration of triglycerides • Electrocardiogram
Recommended tests Fundoscopy Carotid ultrasound Echocardiogram Quantitative proteinuria (if dipstick test positive) Ankle-brachial BP index Home and 24h ambulatory BP monitoring Laboratory Investigations
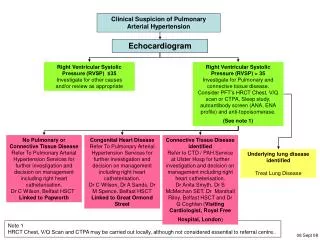
Brain MRI or CT (MRI being generally superior to CT) Silent brain infarcts Lacunar infarction Microbleeds and Whitematter lesions Searching for subclinical organ damage
Fundoscopy In hypertensive with severe disease, only. Searching for subclinical organ damage
Blood vessels Ultrasound scanning of the extracranial carotid arteries A low ankle- brachial BP index signals advanced peripheral artery disease Searching for subclinical organ damage
Heart Echocardiography Left ventricular hypertrophy is considered useful. Geometric patterns Diastolic dysfunction Searching for subclinical organ damage
Kidney Measurement of serum creatinine Creatinine clearance (Cockroft- Gault formula, requiring age, gender body weight) Albuminuria Microalbuminuria Searching for subclinical organ damage
Stratification of CV risk in four categories Blood pressure (mmHg) SBP: systolic blood pressure; DBP: diastolic blood pressure; CV: cardiovascular; HT: hypertension. Low, moderate, high, very high risa refer to 10year risk of a CV fatal or non-fatal event. The term “added” indicates that in all categories risk is greater than average. OD: subclinical organ damage; MS: metabolic syndrome.
Lifestyle measures • weight • body mass index 20-25 kg/m2 • aerobic physical exercise • for 30 minutes per day, ideally on most of days of the week but at least on three days of the week • alcohol consumption • 3 units/day for men and 2 units/day for women • salt intake • <100 mmol/day (<6g NaCl or <2.4 g Na+/day) • saturated fat • reduce the intake of total and • fresh fruit and vegetables • at least five portions/day
Goals of Treatment Clinic BP (mmHg) No diabetesDiabetes Optimal treated BP pressure<140/85<130/80 Audit Standard<150/90 <140/80 Audit standard reflects the minimum recommended levels of blood pressure control. Despite best practice, the Audit Standard will not be achievable in all treated hypertensives. For ambulatory (mean daytime) or home blood pressure monitoring - reducing these targets by ~10/5 is recommended.