Download
1 / 33
350 likes | 445 Views
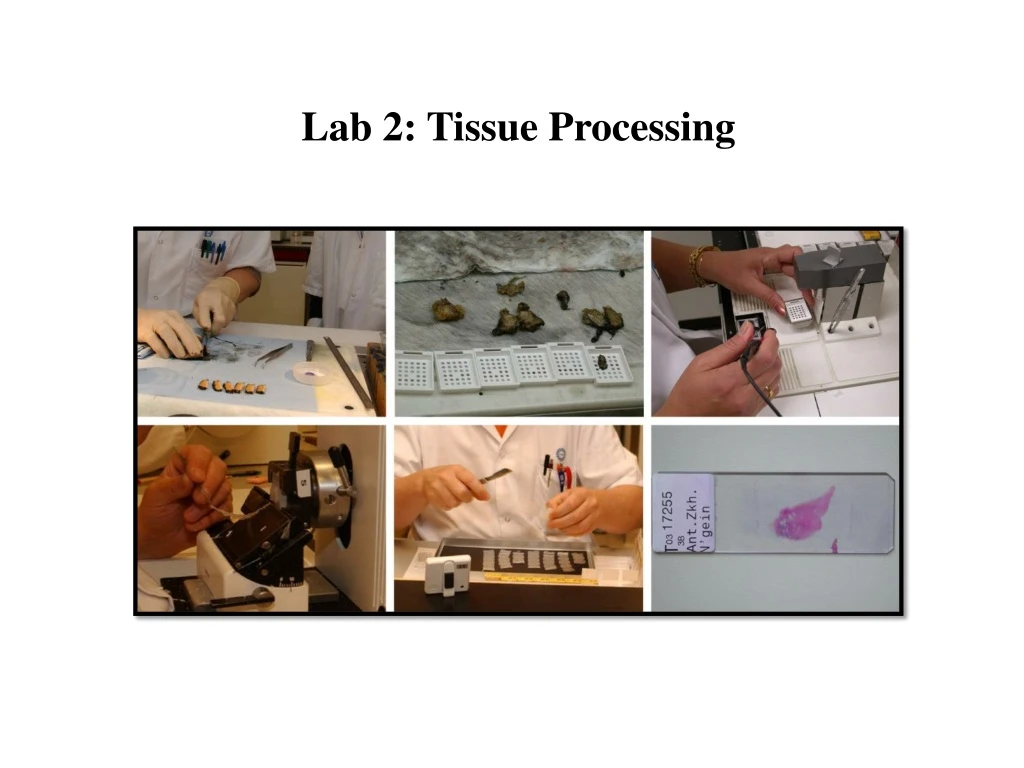
Lab 2: Tissue Processing. Overview. Those who are unfamiliar with histotechnology often ask, “How does a pathologist look at a biopsy under the microscope and diagnose a disease ?

E N D
Overview • Those who are unfamiliar with histotechnology often ask, “How does a pathologist look at a biopsy under the microscope and diagnose a disease ? • The process is long and involved fixation and processing, embedding and microtomy, de-paraffinization and staining, and finally cover slipping.and each sequential step is completely dependent on the previous one. • The majority of surgical tissue is treated with various reagents used to preserve tissue elements (such as nuclei, cytoplasm, and tissue morphology) and prepare the specimen for paraffin embedding and microtomy.
Tissue Processing • It refers to the treatment of the tissue necessary to impregnate it into a solid medium, so that the tissue is rendered sufficiently firm yet elastic for the tissue sections of desirable thickness to be cut on microtome.
Tissue processing can be performed: • Manually (hand processing). • Automated tissue processing machine ( a “tissue processor”):it is used where multiple specimens have to be dealt, it is more convenient and much more efficient than manual processing.
These devices have been available since the 1940’s1 and have slowly evolved to be: 1. Safer in use, 2. handle larger specimen numbers, 3. process more quickly, 4. produce better quality outcomes.
Types of Processors: • The fluid-transfer (or “enclosed”) types where specimens are held in a single process chamber or retort and fluids are pumped in and out as required. • The tissue-transfer (or “dip and dunk”) machines where specimens are transferred from container to container to be processed.
Histopathological Technique • Histopathological technique deals with the preparation of tissue for microscopic examination. • The aim of good histological technique to preserve microscopic anatomy of tissue and make them hard, so that very thin section (4 to 5 micron) can be made. • After staining, the section should represent the anatomy of the tissue as close to as possible to their structure in life.
1. Fixation • This is the process by which the constituents of cells and tissue are fixed in a physical and partly also in a chemical state so that they will withstand subsequent treatment with various reagents with minimum loss of architecture. • This is achieved by exposing the tissue to chemical compounds, call fixatives.
Mechanism of action of fixatives • Most fixatives act by biodegradable enzymes that perform a proteolysis which then form a sponge or meshwork, tending to hold the other constituents. • Good fixative is most important factors in the production of satisfactory results in histopathology. • No fixative will penetrate a piece of tissue thicker than 1 cm.
Properties of an ideal fixative: 1. Prevents autolysis and bacterial decomposition. 2. Preserves tissue in their natural state and fix all components. 3. Make the cellular components insoluble to reagent used in tissue processing. 4. Preserves tissue volume. 5. Avoid excessive hardness of tissue. 6. Allows enhanced staining of tissue. 7. Should be non-toxic and non-allergic for user. 8. Should not be very expensive.
Factor affecting fixation: 1. Size and thickness of piece of tissue. 2. Tissue covered by large amount of mucous fix slowly. 3. The same applies to tissue covered by blood or organ containing very large amount of blood. 4. Fatty and lipomatous tissue fix slowly. 5.Correct choice of fixatives. 6. Fixation is accelerated by maintaining temperature around 60Co.
Formaldehyde • The most commonly used fixative is formalin. • It is prepared by mixing 40% formaldehyde gas in 100w/v of distilled water. • Routinely, 10% formalin is used. Mechanism of action • It forms cross links between amino acids of protein thereby making them insoluble.
Advantages: 1. Rapid penetration. 2. Easy availability & cheap. 3. Does not overharden the tissue. 4. Fixes lipids for frozen sections. Disadvantages: 1. Irritant to the nose, the eyes and mucus membranes. 2. Formation of precipitate of paraformaldehyde which can be prevented by adding methanol. 3. Formation of black formalin pigment, Acid formaldehyde hematin.
Alcohol (Ethyl Alcohol) • Absolute alcohol alone has very little place in routine fixation for histopathology. • It acts as a reducing agents, become oxidized to acetaldehyde and then to acetic acid. • Advantages: • Alcohol penetrates rapidly in presence of other fixative hence in combination e.g. Carnoy's fixative is used to increase the speed of tissue processing. • Ethanol preserves some proteins in relatively undenatured state so that it can be used for immunofluorescence or some histochemical methods to detect certain enzymes. • Methyl alcohol is used for fixing blood and bone marrow smears. • Disadvantages: • It is slow to penetrate, hardens and shrinks the tissue.
Acetone • Cold acetone is sometimes used as a fixative for the histochemical demonstration of some tissue enzymes like phosphatases and lipases. • Its mode of action as fixative is similar to that of alcohol.
Mercuric Chloride (HgCl2) Advantages: -It penetrates rapidly without destroying lipids. Disadvantages: -It causes shrinkage of the tissue if it used alone. -It brings about precipitation of the proteins. -It neither fixes nor destroys carbohydrates. Note: Treatment of the tissue with mercuric chloride brings out more brilliant staining with most of the dyes.
Picric acid Advantages: -It penetrates well and fixes rapidly. Disadvantages: -It produces marked cells shrinkage hence it is not used alone. -It precipitates proteins and combines with them to form picrate's some of the picrate's are water-soluble so must be treated with alcohol before further processing where the tissue comes into contact with water. Note: All the tissues fixed in picric acid containing fixatives should be thoroughly washed to remove the yellow discoloration to ensure proper staining of tissue sections. • If the fixative is not removed by washing thoroughly with time even the embedded tissue loses its staining quality.
Potassium Dichromate • It fixes the cytoplasm without precipitation. • Valuable in mixtures for the fixation of lipids especially phospholipids. • Used for fixing phosphatides and mitochondria. • Note: • Thorough washing of the tissue fixed in dichromate is required to avoid forming an oxide in alcohol which cannot be removed later.
2. Dehydration • Tissues are dehydrated by using increasing strength of alcohol; e.g. 50%, 70%, 90% and 100%. • The duration for which tissues are kept in each strength of alcohol depends upon the size of tissue, fixative used and type of tissue; • e.g. after fixation in aqueous fixative delicate tissue need to be dehydrated slowly starting in 50% ethyl alcohol directly whereas most tissue specimens may be put into 70% alcohol. • Delicate tissue will get high degree of shrinkage by two great concentration of alcohol. • Note: If the water is one of the fixative components must be the work of dehydration step after the fixation process while the water was not a contents do not need to perform this step.
3. Clearing • During dehydration water in tissue has been replaced by alcohol. The next step alcohol should be replaced by paraffin wax. • As paraffin wax is not alcohol soluble, we replace alcohol with a substance in which wax is soluble. • This step is call clearing.
Types of Wax employed for Impregnation: 1. Paraffin wax 2. Water soluble wax 3. Other material, like colloidin, gelatin, paraplast etc. Paraffin wax is used routinely. It has hard consistency, so section of 7 micron thickness can be cut.
4. Blocking • Impregnated tissues are placed in a mould with their labels and then fresh melted wax is poured in it and allowed to settle and solidify. • Once the block has cooled sufficiently to form a surface skin it should be immersed in cold water to cool it rapidly. • After the block has completely cooled it is cut into individual blocks and each is trimmed.
5. Decalcification • It refers to • The loss of calcium salts from a bone or tooth. • OR the process of removing calcareaous matter. • Decalcification process should satisfy the following conditions: • Complete removal of calcium salts. • Minimal distortion of cell morphology. • No interference during staining.
Factors affecting rate of Decalcification: 1. Concentration of decalcifying solution: Increased concentration of the decalcifying agent fastens the reaction. 2. Temperature: The rate of decalcification increases with rise of temperature. 3. Density of bone: Harder bone takes longer time to decalcify. 4. Thickness of the tissue: Small tissue pieces decalcify earlier. 5. Agitation: Agitation increases the rate of decalcification.
Decalcification methods • Acid decalcifying agents The commonest method of decalcification is dissolving calcium salts in an acid solution. Some of the acid decalcifying agents are (Nitric acid, Formic acid and Trichloroacetic acid) 2. Ion exchange resins with acid and decalcifying fluids The removal of calcium ions from the decalcifying fluid by the resins leads to quicker and more efficient decalcification.
3. Electrolytic decalcification • It is the speedier decalcification without damage to cytological features and staining. 4. Chelating agents • EDTA is a chelating agent, it is a white crystalline powder soluble in distilled water to about 20%. • As a decalcifying agent it combines with calcium ions to form soluble, non-ionized compound. • The volume of solution for decalcifying should be 150 times that of the tissue. • The solution should be renewed every 5to7 days during decalcification.
Methods of determining optimum decalcification • Specimens should NOT be crowded together and should NOT contact the bottom of container in order to provide complete decalcification. • Over decalcification can also permanently damage specimen. • The following procedure help determine the correct end-point of decalcification. • X-ray (the most accurate way). • Chemical testing (accurate). • Physical testing (less accurate and potentially damage of specimen).
Chemical testing • Use equal parts of the 5% ammonium hydroxide solution and the 5% ammonium oxalate solution. • Procedure: 1. Insert a pipette into the decalcifying solution containing the specimen. 2. Withdraw approximately 5 ml of the hydrochloric acid/formic acid decalcification solution from under the specimen and place it in a test tube. 3. Add approximately 10 ml of the ammonium hydroxide/ammonium oxalate working solution, mix well and let stand overnight. 4. Decalcification is complete when no precipitate is observed on two consecutive days of testing. Repeat this test every two or three days.
Physical Tests • It includes: • Inserting a pin, razor, or scalpel directly into the tissue. (The disadvantage of inserting a pin, razor, or scalpel is the introduction of tears and pinhole artifacts). 2. Bending the specimen. (It is safer and less disruptive but will not conclusively determine if all calcium salts have been removed). • After checking for rigidity, wash thoroughly prior to processing. • Note: If paraffin embedded bones are not decalcified fully, one can soak the paraffin blocks in the same decalcification solution for a few minutes before cutting. This is usually helpful.