Download
1 / 13
130 likes | 146 Views
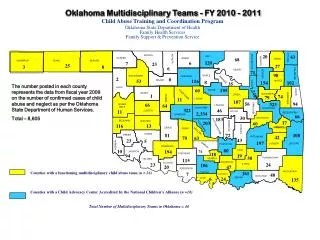
OHPRP is a program designed to support and monitor medical and allied health professionals experiencing difficulty with substance abuse. It works cooperatively with the state board of medical licensure to restore a physician's ability to practice safely and protect the public.

E N D
Oklahoma’s Health Professional Recovery Program Ken King, CAE OSMA Executive Director
Oklahoma’s Substance Abuse Recovery Program • Chemical dependency & alcoholism is a disease that occurs in about 10% of the general population. • Rate within the healthcare profession is higher, occurring in between 10-15%. • OHPRP works cooperatively with the state board of medical licensure to restore a physician’s ability to practice safely & protect the public.
OSMA’s OHPRP Program-1983-1997 • Since 1983, OSMA has provided services to physicians with alcohol abuse and chemical dependence issues. • OHPRP is an outreach program designed to support & monitor medical & allied health professionals experiencing difficulty with substance abuse. • Employs 1 full time & 2 part time physician medical directors to administer program.
OHPRP (cont.) • Program is designed to coordinate and monitor intervention, evaluation, treatment and continuing care of impaired physicians. • Take referrals from: • Hospital staffs • Medical groups • Colleagues • Families • Licensing Boards
Treatment vs. Discipline • OSMA’s Rehabilitative Approach: • Alcoholism declared a disease in 1948 & chemical dependency in 1953 by the AMA • Evidence is clear that treatment is a much more effective method of dealing with problem than trying to discipline the behavior
OHPRP’s Relationship with Medical Board • OHPRP is independent of the Ok. State Board of Medical Licensure & Supervision (OBMLS). • However, documentation of participation & compliance with OHPRP’s monitoring program can be essential in helping maintain and/or restore licensure. • OK Medical Practice Act requires an MD to report to the Board if there is a, “prudent basis to suspect that another physician is practicing while impaired by substance abuse or is habitually drunk or on drugs and is physically/mentally unstable.”
OHPRP’s Relationship with Medical Board (cont.) • While there is no formal arrangement with the OBMLS, if a physician with a substance abuse problem signs an agreement to participate in OHPRP, remains in compliance and there are no allegations of patient harm, there is a reasonable chance that the Board will not have to be involved.
OHPRP Program (cont.) • Since the mid-1980s, more than 750 physicians have successfully completed treatment and returned to work. • This equates to returning over six University of Oklahoma medical school graduating classes to the physician workforce. • Currently monitoring 125 MDs, DOs, PAs, and Dentists
PLICO Support for OHPPLiability data for 14 years • MD’s in OHPRP Program 9/83 to 3/97 (258): Pre-Discovery Recovery # of OHPRP phys. w/ claims 89 39 # of claims 248 52 Paid/reserved for claims 8,017,000 307,600 Tot. MDs covered 4/2/94: 3,933 Paid/reserved for claims: 156.8 million
Comparison of Medical Malpractice Claims • 1980-1995 Pre-treatment Post Treatment • Identified 94 94 Physicians w/ claims • Avg. claim payment $37,382 $5,711 • Annual proj. pymt. $932,248 $70,012 • Proj. est. ann. savings: $903,236
Conclusions • OHPRPs value Over 750 physicians have been successfully treated and returned to work Reputation for collaborating closely with the medical licensing boards to protect the public Reinforces Board reputation for being firm and fair Refuted plaintiff’s bar argument that boards don’t protect patients
Conclusions • OHPRP Key Components: • Good working relationship with licensing boards • Identify those who just don’t get it • Monitoring is a 2-5 year contract: • Drug and alcohol screening every 3-4 days • Random testing • Caduceus & AA required • Support rather than Punishment