Download
1 / 19
190 likes | 285 Views
The Prevalence of Autism in the In-patient Population of Norristown State Hospital. Donielle N. Johnson LDI Summer Undergraduate Minority Research Program August 8, 2008. http://farm3.static.flickr.com/2305/2385952133_15eb5a44a7.jpg?v=0. Purpose.

E N D
The Prevalence of Autism in the In-patient Population of Norristown State Hospital Donielle N. Johnson LDI Summer Undergraduate Minority Research Program August 8, 2008
http://farm3.static.flickr.com/2305/2385952133_15eb5a44a7.jpg?v=0
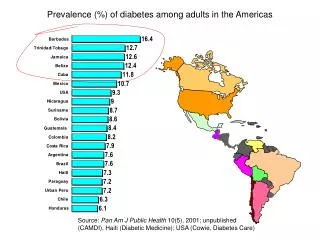
Purpose • To estimate the prevalence of Autism Spectrum Disorders (ASD) among patients at Norristown State Hospital • To learn more about ASD in in-patient psychiatric populations • To better understand differential diagnoses in adults
Issues That Contextualize the Project • Concern about ASD diagnosis is increasing • We remain unaware of whether the awarenessof ASD is increasing due to new technology and attention or whether the actual prevalenceof ASD is increasing in our communities • Understanding and differentiating between similar symptoms such as negative symptoms of schizophrenia and ASD’s characteristic social withdrawal is important yet fairly unexplored
Why Adults? • Prevalence of adults with ASD offers insight into two situations: • If ASD prevalence is increasing, fewer adults should have ASD than children • If awareness of ASD is increasing, the number of adults with undiagnosed ASD is unknown and significant • Potential for adults to live in psychiatric facilities since: • Symptoms between ASD and other psychiatric disorders can be nearly indistinguishable • Adults with ASD generally do not live alone without assistance
Patient Demographics at Norristown State Hospital • 350 civil commitment patients • 69% male • 61% white, 34% black, 3% Latino, 2% Asian • Average Age 49 yrs, range of 20-82 • 62% completed high school (4% unknown) Slide Courtesy of Lindsay Lawer and David Mandell
Phase One • Attempt to obtain sufficient information to determine the prevalence of ASD at NSH using the Social Responsiveness Scale (SRS) and record reviews
Phase One Instrument- SRS • Quantitative measure of autistic traits • Uses deficits in all three areas required by the DSM-IV-TR for an ASD diagnosis Slide Courtesy of Lindsay Lawer and David Mandell
More on SRS • Scores can range from 0 to 195 • Population mean is about 31 • Score > 85 for children age 4-18 has 98% specificity for a clinical diagnosis of PDD-NOS, Asperger’s disorder or autistic disorder • Scores 80 to 100 consistent with mild PDD-NOS, Asperger’s, or negative symptoms of Schizophrenia Slide Courtesy of Lindsay Lawer and David Mandell
22% 21% Phase One Outcome: 21% of in-patients have SRS scores highly specific for Autistic Disorder; 22% have scores consistent with HFA SRS scores mean=75; SD= 33 Slide Courtesy of Lindsay Lawer and David Mandell
Patients with higher SRS scores usually had • Earlier age of onset of problems • Not began high school • Poor overall functioning • Abnormal movements (as judged by AIMS assessment) • Gastrointestinal problems • Their diagnoses were more likely to be • Mental retardation • (Chronic) Undifferentiated schizophrenia • “Other” disorders and psychoses Slide Courtesy of Lindsay Lawer and David Mandell
Phase II- In Progress • Autism Diagnostic Interview Revised (ADI-R) • Phone administered diagnostic instrument focusing on development • SRS and the ADI-R correlation is greater than 0.64 • In-depth historical chart review • Clinical interview • Neurobehavioral assessments of patients
Chart Reviews and Family Calls • My biggest contribution to the current research • Main route to gaining historical insight into patient’s developmental history and onset of psychiatric abnormalities • Many patients lack either living or involved relatives that can speak to childhood development and any problems experienced • Uncertain how much hospitalization exacerbates social deficits • Need to examine patient history and behaviors prior to hospitalization • DSM criteria states ASD onsets before age of 3
Ward Chart More current Initial assessments and diagnoses as well as most recent • Historical Chart • Developmental history • Number of hospitalizations • Past diagnoses • Recurrent problems • Techniques used for treatment • For patients that have been institutionalized as children chart has these diagnoses as well
Family Calls and the ADI-R • “Gold standard” diagnostic family interview instrument • Relative reports on childhood presentation and interaction with others • Must have spent time with individual before 7th birthday
Family and Patient Concerns • Tend to express same type of concerns when asked to participate in the study • Tend to inquire about • Change in medication • Change in length of stay/delay in discharge • Confidentiality • Exploitation of family members for research
Implications • ASD may be very prevalent among in-patients at NSH • could be missed in this population or be co-morbid with disorders • ASD may be exacerbated by hospitalization • Development of methods for diagnosis and treatment ASD in adults
Special Thanks To: • David Mandell • Lindsay Lawer • Kira Branch
Special thanks to the following organizations for their generous support: • The University of Pennsylvania Provost’s Diversity Fund • The Center for Health Equity Research and Promotion (CHERP) • Pennsylvania Department of HealthOffice of Health Equity



![Projected Senior Population Growth in the State of Michigan [Infographic]](https://cdn4.slideserve.com/7250670/slide1-dt.jpg)