Download
1 / 20
200 likes | 399 Views
Unusual Brain Lesion with a Usual Cause. Ryan Frederiksen MD, Sean Snodgress MD, Benjamin Kianmahd MSIV Department of Radiology Santa Barbara Cottage Hospital. Clinical History: Patient A. 36 year old right handed male with no prior medical history Found unresponsive at gas station

E N D
Unusual Brain Lesion with a Usual Cause Ryan Frederiksen MD, Sean Snodgress MD, Benjamin Kianmahd MSIV Department of Radiology Santa Barbara Cottage Hospital
Clinical History: Patient A • 36 year old right handed male with no prior medical history • Found unresponsive at gas station • No history of drug abuse, trauma, hypertension, hypercoaguable state or significant family history • Physical Exam: GCS 8 • Labs: within normal limits except for BS > 500
Imaging: Patient A Initial Head CT Day 1: Normal. Head CT Day #1 Initial Head CT was normal
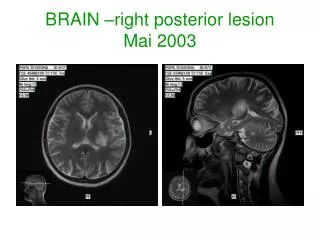
Imaging: Patient A MRI DWI MRI ADC MRI Day 2:Bilateral thalamic infarcts.
Imaging: Patient A Head CTA Day 2:Bilateral thalamic infarcts;CTA portion was normal. Head CT Day #1 Initial Head CT was normal
Imaging: Patient A Head CT Day 3:Hemorrhagic thalamic infarcts. Head CT Day #1 Initial Head CT was normal
Clinical History: Patient B • 85 year old male with history of hypertension and GERD • Presented to PMD with 5 day history of ataxia and double vision • Physical Exam: leftward ataxic gait, bilateral horizontal nystagmus, no focal sensory or motor deficits • Labs: LDL 151
Imaging: Patient B MRI FLAIR MRI DWI MRI Day 5 of Symptoms: Bilateral thalamic infarcts.
Bilateral Thalamic Infarcts • Broad differential diagnosis • Venous occlusion: vein of Galen, straight sinus, bilateral internal cerebral veins • Diffuse astrocytoma • ADEM • Arterial ischemia: artery of Percheron
Discussion: Background • These two cases demonstrate an anatomic variant • Occlusion of the artery of Percheron results in a characteristic pattern of infarct • Infarct of the bilateral paramedian thalamus with or without midbrain involvement
Discussion: Background • The thalamus’ blood supply is usually supplied by: • multiple perforator vessesls originating from the posterior communicating artery • the P1 and P2 segments of the posterior cerebral arteries
Discussion: Background • The anterior region is supplied by • the polar (thalamotuberal) arteries, arising from the posterior communicating artery • The paramedian region is supplied by • the paramedian (thalamoperforating) arteries which originate from the P1 segment of the posterior cerebral artery • The inferolateral region is supplied by • the thalamogeniculate arteries which arise from the P2 segment of the posterior cerebral artery • The posterior region is supplied by • the posterior choroidal arteries, which originate from the P2 segment of the posterior cerebral artery.
Discussion: Background • The paramedian arteries supplying the thalamus and midbrain exhibit the greatest amount of variability • According to Percheron, there are three variations • This exhibit focuses on a specific anatomic variant of the paramedian arteries, known as the Artery of Percheron
Discussion: Paramedian Thalamic Blood Supply Variations 2 • Many perforating arteries from the P1 segment of the PCA; the most common • A single artery from the P1 segment; the artery of Perheron • An arcade of perforating arteries from both PCAs
Discussion: Artery of Percheron 3 A single dominant thalamoperforating artery supplying the bilateral medial thalami with variable contribution to the rostral midbrain
Discussion • Common physical exam findings • Oculomotor palsy (76% of patients) • Mild gait ataxia (67%) • Deficits of attention (63%) • Fluency and error control (59%) • Learning and memory (67%) • Behavior (67%)
Discussion • One retrospective study identified four patterns of artery of Percheron infarcts • Bilateral paramedian thalamic with midbrain (43%) • Bilateral paramedian thalamic without midbrain (38%) • Bilateral paramedian thalamic with anterior thalamus and midbrain (14%) • Bilateral paramedian thalamic with anterior thalamus without midbrain (5%)
Conclusion The artery of Percheron is one of the few examples where a cerebral blood vessel supplies structures on both sides of the midline!
References • Lazzaro NA, et al. Artery of Percheron infarction: imaging patterns and clinical spectrum. AJNR Am J Neuroradiol. 2010 Aug;31(7):1283-9. Epub 2010 Mar 18. • Matheus MG, et al. Imaging of acute bilateral paramedian thalamic and mesencephalic infarcts. AJNR Am J Neuroradiol. 2003 Nov-Dec;24(10):2005-8. • Mujeeb, S, et al. Symmetric bilateral thalamic infarcts: a rare complication of cardiac catheterization. The Internet Journal of Cardiology. 2009 Vol 7; No 1.