Download
1 / 141
1.41k likes | 1.48k Views
MANAGING THE ARCH CIRCUMFERENCE . Diagnosis and Treatment Planning. Introduction. Managing the arch circumference is a formidable task. Decisions are frequently tentative. Learning goal is not sophistication; but basic, foundational knowledge.

E N D
MANAGING THE ARCH CIRCUMFERENCE Diagnosis and Treatment Planning
Introduction • Managing the arch circumference is a formidable task. • Decisions are frequently tentative. • Learning goal is not sophistication; but basic, foundational knowledge. • Build on knowledge through electives, post-doctoral education, and practice experience.
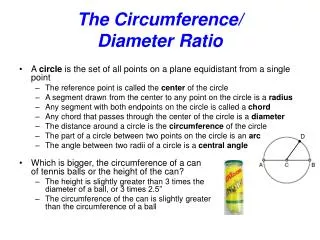
Arch Circumference The distance from the distal of the second primary molar (or mesial surface of the first permanent molar) on one side of the arch to that same surface on the opposite side of the arch.
Arch Circumference It is the space which during the primary dentition is occupied by the 10 primary teeth, and the space that will be available for the eruption of the 10 succendaneous teeth.
Arch Circumference • Arch circumference is relatively unaffected by growth. • It increases slightly with the more anterior (procumbent) positioning of the permanent incisors on their eruption, but it decreases as a result of the mesial migration of the first permanent molars during the canine-premolar transition. (“leeway space”)
Two Goals. . .in managing the arch circumference • 1. The arch circumference’s integrity is maintained in order that the child’s inherent potential to erupt the succedaneous teeth in normal arch alignment is realized. • 2. The succedaneous teeth are assisted in erupting into as normal an arch alignment as possible within the constraints of the size of the arches and the size of the tooth mass.
Two Problems . . .in managing the arch circumference • 1. Available arch circumference may be lost as a result of pathology, and • 2. A discrepancy may exist between the size of the succedaenous teeth and the amount of arch circumference available.
Physiologic Forces A tooth is maintained in its correct relationship by the action of several forces. An alteration in these forces can alter the relationship among the teeth.
Physiologic Forces Of primary concern is the mesial migration of the first permanent molar; any mesial movement, by definition, reduces arch circumference.
Primary Causes of Loss of Arch Circumference • Extraction of posterior primary teeth due to pulpal pathology. • Interproximal caries
Additional Causes of Loss of Arch Circumference • Ankylosis of primary tooth • Ectopic eruption of the first permanent molar
Anklyosis Ankylosis An aberration in the eruption of teeth in which the continuity of the periodontal ligament becomes compromised, with fusion of the cementum and bone at one or more locations. Results in the tooth being “submerged” relative to the occlusal plane. Adjacent teeth may tip into space, resulting in loss of arch circumference.
Ectopic Eruption Ectopic Eruption Eruption of first permanent molar into the root of the second primary molar. Prevalence 2-3% Generally self-correcting, but can cause loss of second primary molar if not corrected, with first permanent molar positioning itself anteriorly, with resultant loss of arch circumference.
Inadequate Arch Circumference • It is frequently the case that a practitioner preserves the integrity of the arch circumference and yet a malocclusion develops due to a basic discrepancy between the size of the succedaneous teeth (mesial-distal width) and the amount of arch circumference available for their eruption. • This is frequently stated as a “tooth size/arch circumference discrepancy.” • Plainly stated, the child’s “teeth are too big for the size of the jaws.”
Inadequate Arch Circumference • The first manifestation of this problem is when the first succedaneous teeth erupt, the mandibular permanent incisors. • They may be crowded, rotated, blocked out, or in their eruption cause the exfoliation of one or both of the primary canines; this is referred to as ectoptic eruption of the lateral insisor(s).
Management of the arch circumference includes the management of the inadequacy of its circumference relative to the size of the succedaneous tooth mass.
DIAGNOSTIC CONSIDERATIONS In Managing the Arch Circumference
Diagnostic Data Base • Diagnosis and treatment can be complex, especially in the mixed dentition. • A valid data base must be gathered in a systematic manner. • Data Base: • Case History • Oral Examination • Radiographic survey and in the mixed dentition • Diagnostic Casts and a Space Analysis
Questions To Be Answered From The Data Base 1. What is the patient’s profile? 2. Has there been premature loss of teeth and/or does it appear that teeth present will have to be extracted prematurely? 3. What is the occlusal development? 4. Is there a discrepancy between the available arch circumference and the size of the permanent succedaneous teeth?
What is the patient’s profile? • Important in determining facial growth patterns • Can be determined in a preliminary (non-definitive) manner, that is, without the exposure of a cephalogram, by clinically relating the bony aspects of the maxilla and mandible to one another and the cranial base
What is the patient’s profile? This evaluation is accomplished by: • palpating the basal bone above the roots of the maxillary incisors -- Point A on a cephalogram; • palpating the basal bone below th roots of the mandibular incisors -- Point B on a cephalogram; • palpating the nasal bone -- Nasion on a cephalogram.
What is the patient’s profile? • Ideally, the bony landmarks should be in a direct line relationship with one another, an orthognathic profile. • A (developing) skeletal Class II is characterized by a retrognathic mandible. • A (developing) skeletal Class III is characterized by a prognathic mandible.
Orthognathic Profile 1. Cranium 2. Maxilla 3. Maxillary Dentition 4. Mandibular Dentition 5. Mandible
What is the patient’s profile? • In the mixed dentition, children with a developing retrognathia or prognathiashould be referred to a specialist for consultation in the context of the generalist managing the arch circumference, as management of the arch circumference exists in the context of a larger skeletal problem. However, it is generally always advisable to maintain the integrity of the arch circumference, even in the context of an overarching skeletal problem. • Space management by the generalist alone is most appropriate and successful in the patient with an orthognathic profile.
Has there been premature loss of primary teeth and/or does it appear that primary teeth present will have to be prematurely extracted? • Which teeth?Arch circumference loss is greater with second primary molars that with first primary molars. • Has there already been loss of arch circumference?If not, management man involve simple maintenance of available space. In instances where you remove a tooth and all other factors indicate a need for space maintenance, the appliance should be placed immediately. Watchful waiting for space closure following extraction is never indicated!
Premature Loss? • If space loss has already occurred: • What is the magnitude of the loss? If it proves to be necessary to regain lost arch circumference, different appliances are used depending on the magnitude of the loss. • Is there still adequate space remaining to permit eruption of the succcedaneous tooth? If so, regaining lost arch circumference may be unnecessary.
Premature Loss? • Is it possible that additional arch circumference could be lost?Space closure following extraction of primary molars is generally related to the position and eruption of the first permanent molar. In the late mixed dentition it may be more related to the position and eruption of the second permanent molar. Because of this, space loss may be immediate or delayed. However, it is generally found that significant amounts of space loss will occur within the first six months following extraction. Additional increments of loss may occur at periods associated with the eruption of the permanent molars.
Premature Loss? • Is the succedaneous tooth present?The congenital absence of the succedaneous tooth (or teeth) may affect your decision of how to manage the available arch circumference. The second premolars are common congenitally missing teeth. An evaluation of the presence or absence of this tooth is an important consideration. The second premolar is also highly variable in the initiation of its calcification. Formation can begin as late as 8 years of age, so be wary of jumping to conclusions.