Download
1 / 18
180 likes | 444 Views
Muscles and Movement. Dan Foster, PhD, ATC January 7, 2010. Rothbart B, May 2009. Athletic Training Assessment. Skilled Movement Deficiency Rule-out life & limb threatening injuries or Rule-out referral issues or Functional status.

E N D
Muscles and Movement Dan Foster, PhD, ATC January 7, 2010 Rothbart B, May 2009
Athletic Training Assessment • Skilled Movement Deficiency • Rule-out life & limb threatening injuries • or • Rule-out referral issues • or • Functional status Philosophy of approach for deficiencies and functional status: minor alterations in precision of movement lead to injury and pain, caused by changes in muscle length, strength, stiffness, and movement patterns
Key Elements • Assessment of alignment • Indicates possible muscle length changes and joint alignment • Interfere with optimal movement • Movement patterns • Specific muscle length and strength testing Borstad J, Phys Ther, 2006 Whyte E, Gait & Post, 2010 Garner B, BioMed Engineer, 2004
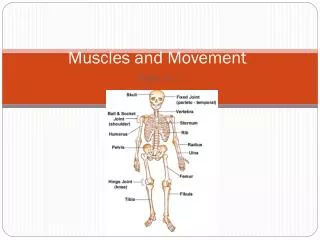
Scapular & Humeral Alignment • Vertebral border parallel to spine • ~ 3 in. away • Between T2 – T7 • Flat on chest wall • Rotated 30o anteriorly • Less than 1/3 protruding • Cubital fossa forward • Humerus vertical Garner B, BioMed Engineer, 2004 Kibler W, AJSM, 1998
Alignment Issues • Downwardly rotated
Scapular Motions • Scapula variable during first 30o abd or 60o flex • Remaining 120o Humeral and 60o Scapular • Timing often 140o Humeral flex when scapula stops Inman V, JBJS, 1944
Muscle Physiology and Control • Strength • Length • Stiffness • Timing
Muscle Strength • Capacity • Fiber number • Contractile elements • Hypertrophy/Atrophy • Arrangement • Series/Parallel • Length of fibers • Configuration • Overlapped, lengthened, disrupted Tipton C, Am J Physiol, 1970 Wilkie D, Br. Med Bull, 1956
Muscle Length • Prolonged elongation • Strain injury and continuous tension • Sustained stretching Kendall F, 1993
Muscle Stiffness • Change in tension per unit change in length • Contributes to movement patterns • Active and passive stiffness • A factor in compensatory motion in contiguous joints Sahrmann S, 2002
Movement Timing • Altered recruitment patterns • Upper trapezius dominance • Learned • Preferred pattern due to pain • Delayed or insufficient action • Stabilizing muscle causes movement
Case • 16 YO ♀ swimmer with B shoulder pain R>L • Cumul pain occurs in flex & abd at ~100o • Swimmer since 6, ranked high at one time • Works hard, weight training & swim despite • 5’7” 127# • Slight thoracic kyphosis, weak abs • B shoulder girdle elevation, arms abd
B scapular abd • Humerus glides sup, at 120o flex humerus med rotates/pop, glide sup on return to neutral • Trunk ext on shoulder flex to counterbalance • If trunk is stabilized, flex is limited • Trapezius & Rhomboids are short (hard to determine) • Deltoid & Supraspinatus are short • Lat rotators are stiff • Lower & mid Trapezius are weak • Deltoid becomes dominant on ER – Humeral ext, winging, and humeral head glide sup • On IR & ER immediately initiates scapular motion • Serratus is weak and wings in quadruped position
Diagnosis? • Impingement • Supraspinatus tendinopathy • Subacromial or subdeltoid bursitis • Bicepital tendinopathy • Humeral superior glide – primary • During shoulder flexion with elbow flexion sx ↓ • Scapular abduction - secondary
Treatment • Primary emphasis • Stretch deltoid and decrease dominance • Improve control of trapezius and serratus ant • Learn how to control IR/ER without other motions (supine) • Target infraspinatus and teres minor (prone & standing) • Control scapula and sup glide on IR (prone)
Outcome • Within 4 weeks (no swimming) • Arms at side during rest • Arms flex without pain to 180 and w/o moving trunk • No medial rotation with popping • Tolerates 4 pounds of load • Ready to step up her activity and resume swimming when she can go through her stroke without popping
Summary • Minor alterations in precision of movement lead to injury and pain, caused by changes in muscle length, strength, stiffness, and movement patterns • The influence of multiple muscle interactions acting on multiple joints in functionally oriented tasks is where we might go with deficiency screening and rehab recovery