Download
1 / 35
350 likes | 833 Views
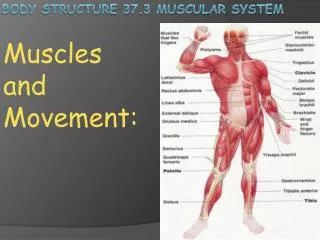
Option B – Muscles Movement and Fitness. B.1.1 State the roles of bones, ligaments, muscles , tendons and nerves in human movement . B1 - Muscles and movement.

E N D
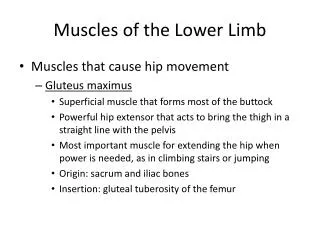
B.1.1 State the roles of bones, ligaments, muscles, tendons and nerves in human movement. B1 - Muscles and movement Bonesprovide the structure onto which soft tissue is built, they provide protection for internal organs, as well as provide a system of levers that allow for movement by way of muscular contraction. Ligaments hold bones together Nerves signal muscles to contract. Musclesdo the work….They pull against bones to provide movement. Tendons join muscles to bones. http://www.aclsolutions.com/images/Seif_knee%20anatomy02.jpg http://www.human-body-facts.com/images/human-body-muscle-diagram.jpg http://jagpower.blogspot.com/2011/10/bones-provide-structure-onto-which-soft.html httphttp://www.ehrenchiropractic.com/nervous_sys.jpg://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/8956.jpg
B.1.2 Label a diagram of the human elbow joint, including cartilage, synovial fluid, joint capsule, named bones and antagonistic muscles (biceps and triceps).Outline the functions of the structures in the human elbow joint named. Bending the elbow diagram - put the numbers in the right places! 1. Ulna 2. Radius 3. Contracted biceps brachii muscle 4. Relaxed triceps muscle 5. Humerus Straightening the elbow diagram - put the numbers in the right places! 1. Radius 2. Relaxed biceps brachii muscle 3. Humerus 4. Contracted triceps muscle 5. Tendon 6. Ulna 1 1 2 2 3 3 4 4 5 5 5 5 5 6 http://campaigns2.axappphealthcare.co.uk/medical-encyclopaedia/bending-the-elbow
Match the description on the right with the part on the left : • Holds the bones together. • Provides a very smooth surface to reduce friction. • Acts as a lubricant. • Secretes and holds in synovial fluid
B.1.4 Compare the movements of the hip joint and the knee joint. 1 2 3 Click the circles for the 3 types of movement available in a hip: Flexion/extension/hyperextension Adduction/abduction Circumduction Click the patella for the types of movement available in the knee.
B.1.5 Describe the structure of striated muscle fibres, including the myofibrils with light and dark bands, mitochondria, the sarcoplasmic reticulum, nuclei and the sarcolemma.
B.1.6 Draw and label a diagram to show the structure of a sarcomere, including Z lines, actin filaments, myosin filaments with heads, and the resultant light and dark bands.
B.1.7 Explain how skeletal muscle contracts, including the release of calcium ions from the sarcoplasmic reticulum, the formation of cross-bridges, the sliding of actin and myosin filaments, and the use of ATP to break cross-bridges and re-set myosin heads. Click on the image to go to a great animation that guides you through how a muscle contracts and has great questions to help you see how much you’ve learned. (alternatively click the hyperlink below…) http://www.brookscole.com/chemistry_d/templates/student_resources/shared_resources/animations/muscles/muscles.html http://highered.mcgraw-hill.com/sites/0072495855/student_view0/chapter10/animation__action_potentials_and_muscle_contraction.html http://www.blackwellpublishing.com/matthews/myosin.html Some other animations you might try…. http://www.youtube.com/watch?v=CepeYFvqmk4
B.1.8 Analyse electron micrographs to find the state of contraction of muscle fibres. If electron micrographs of a relaxed and contracted myofibril are compared it can be seen that: 1. Each sarcomere gets shorter (Z-Z) when the muscle contracts, so the whole muscle gets shorter. 2. But the dark band, which represents the thick filament, does not change in length. This shows that the filaments don’t contract themselves, but instead they slide past each other. http://click4biology.info/c4b/11/hum11.2.htm#8
B.2.1 Define total lung capacity, vital capacity, tidal volume and ventilation rate. Total lung capacity : volume of air in the lungs after a maximum inhalation. : maximum volume of air that can be exhaled after a maximum inhalation. : volume of air taken in or out with each inhalation or exhalation. : number of inhalations or exhalations per minute (this term is used, not breathing rate). Vital capacity Tidal volume Ventilation rate
B.2.2 Explain the need for increases in tidal volume and ventilation rate during exercise. http://www.livestrong.com/article/288393-increase-in-tidal-volume-during-exercise/ Read the article then complete the sentences: When you exercise you need to breath deeper because….. When you exercise you need to breath more often because….. The ventilation and depth are controlled by negative feedback. What is the stimulus? Where is the stimulus detected?
B.2.3 Outline the effects of training on the pulmonary system, including changes in ventilation rate at rest, maximum ventilation rate and vital capacity. http://www.normalbreathing.com/c-effects-of-exercise-on-the-respiratory-system.phpRead the article and try to make a summary table in words rather than numbers…….:
B.3.1 Define heart rate, stroke volume, cardiac output and venous return. Learn these definitions : volume of blood pumped out with each contraction of the heart. : volume of blood pumped out by the heart per minute. : volume of blood returning to the heart via the veins per minute. Stroke volume Cardiac output Venous return
B.3.2 Explain the changes in cardiac output and venous return during exercise. Why does the heart rate need to speed up when you exercise? How is this speed up controlled? What effect will speeding up the heart have on how much blood is pumped out per minute? What effect will pumping more blood out of the heart per minute have on the amount of blood returning (venous return)? Detection of lowered blood pH causes impulses to be sent by the brain to the pacemaker, increasing cardiac output. Contraction of muscles used during exercise squeezes blood in adjacent veins, increasing venous return. Venous return (VR) is the flow of blood back to the heart. Under steady-state conditions, venous return must equal cardiac output (CO) when averaged over time because the cardiovascular system is essentially a closed loop. Otherwise, blood would accumulate in either the systemic or pulmonary circulations. http://wiki.answers.com/Q/What_is_the_effect_of_exercise_on_venous_return#ixzz1niqa1II1
B.3.3 Compare the distribution of blood flow at rest and during exercise. • Blood flow to the brain is unchanged during exercise. Blood flow to the heart wall, skeletal muscles and skin is increased, but blood flow to the kidneys, stomach, intestines and other abdominal organs is reduced. http://www.teachpe.com/anatomy/blood_flow.php But why?
B.3.4 Explain the effects of training on heart rate and stroke volume, both at rest and during exercise. Start here -----> http://www.bbc.co.uk/schools/gcsebitesize/pe/exercise/2_exercise_effectsoftraining_rev1.shtml now explain “why?” Now test yourself by taking the quiz at the end… http://www.bbc.co.uk/apps/ifl/schools/gcsebitesize/pe/quizengine?quiz=2_exercise_effectsoftraining_test&templateStyle=pe
B.3.5 Evaluate the risks and benefits of using EPO (erythropoietin) and blood transfusions to improve performance in sports It is all about oxygen supply to the muscles! The more oxygen you can supply the longer before muscles get tired. If you have maxed out you vital capacity and maxed out you heart efficiency the next thing you can do is increase the amount of oxygen the blood can carry…… one way to do this is to increase the number of red blood cells – and there are 3 ways of doing this; Train at high altitude - http://en.wikipedia.org/wiki/Altitude_training Inject EPO - http://en.wikipedia.org/wiki/Erythropoietin Use a blood transfusion (also called blood doping)- http://en.wikipedia.org/wiki/Blood_doping
B.4.1 Define VO2 and VO2 max. VO2max is the maximum capacity of an individual's body to transport and use oxygen during exercise, which reflects the physical fitness of the individual. The name is derived from V - volume, O2 - oxygen, max - maximum. This instrument measures the amount of oxygen in the air breathed in and compares it with the amount in the air breathed out as the test subject carries out increasing levels of exercise. http://en.wikipedia.org/wiki/File:Ergospirometry_laboratory.jpg
B.4.2 Outline the roles of glycogen and myoglobin in muscle fibres. Glycogen is an glucose storage molecule in muscles. Myoglobin is an oxygen storage molecule in muscles(Like heamoglobin but it remains in the muscle.) http://wikis.lib.ncsu.edu/images/1/19/Hemoglobin.jpg
B.4.3 Outline the method of ATP production used by muscle fibres during exercise of varying intensity and duration. Creatine phosphate can be used to regenerate ATP for 8–10 seconds of intense exercise. Beyond 10 seconds, ATP is produced entirely by cell respiration. As the intensity of exercise decreases and the duration increases, the percentage of anaerobic cell respiration decreases and aerobic cell respiration increases. • Look at the first 1min30secs of this you tube clip: http://www.youtube.com/watch?v=BR3dDO1Sz0E Then look at the side effects in thesecond half of this clip.(Less exciting clip but informative): http://www.youtube.com/watch?v=OzGJnbBay90&feature=related
B.4.4 Evaluate the effectiveness of dietary supplements containing creatine phosphate in enhancing performance. Artificial supplementation of the diet with creatine phosphate increases the amount of the molecule needed to create more ATP quickly and anaerobically. Creatine phosphate is normally readily available in meats and fish. So supplementation may be effective in vegetarians. It is only performance enhancing in sprint sports such as weight lifting and running swimming. Training has no impact on Creatine phosphate levels. Too high creatine phosphate may lead to kidney disease/damage in about 0.1% of people taking supplements.
B.4.5 Outline the relationship between the intensity of exercise, VO2 and the proportions of carbohydrate and fat used in respiration. Energy is primarily supplied from two sources: •Carbohydrates - in the form of glycogen stored in the muscles • Fat - stored around the body During exercise, we use a combination of these energy sources. At a high intensity the main source of energy is carbohydrate and at a low intensity fat is the predominate source. As there is a limit to the amount of carbohydrate that can be stored in the muscles, high intensity work can only be sustained for short periods. We have large stores of fat so low intensity work can be maintained for long periods. • Referenced Material • O'NEIL, T. et al. (2001) Indoor Rowing Training Guide. Concept 2 Ltd, p. 27 • MACKENZIE, B. (2001) Exercise Intensity and Energy Source [WWW] Available from: http://www.brianmac.co.uk/esource.htm [Accessed 13/3/2012]
B.4.6 State that lactate produced by anaerobic cell respiration is passed to the liver and creates an oxygen debt. Often during strenuous exercise, there is not enough oxygen for complete aerobic respiration and anaerobic respiration starts. This produces lactate and carbon dioxide, which causes the further dilation of the arterioles supplying the muscles and so the blood flow to them. Lactate is dangerous because it reduces the pH in cells and decreases the efficiency of the enzymes working inside them. It also causes fatigue and pain (stitch), so it is taken to the liver and converted back to glucose because it is too rich a source of energy to be excreted.
B.4.7 Outline how oxygen debt is repaid. The oxygen debt • Whenever lactate is produced by anaerobic respiration, an oxygen debt is being built up. This debt is paid back at the end of the exercise by breathing more deeply than you would normally need to at rest. • This oxygen is used to convert the lactate to glucose, the haemoglobin to oxyhaemoglobin, oxygenate the myoglobin and supply the higher metabolic rate caused by many organs working harder than usual. • For lengthier exercise, oxygen supply must equal oxygen demand and so an athlete will be more successful the more the muscles are supplied with oxygen. • To increase fitness, you need to train at about 70% of your hearts maximum heart rate for twenty minutes, three times a week. A more intense approach would get quicker results but four or five times a week is the maximum recommended frequency.
B.5.1 Define fitness. • Fitness is the physical condition of the body that allows it to perform exercise of a particular type. - A.Allott – IB Study Guides Biology. However ‘Fitness’ is specific to the type of activity – a swimmer may be very fit to swim but can’t run well as different muscle groups may have been developed and creatine and glycogen storages used.
B.5.2 Discuss speed and stamina as measures of fitness. • Speed is the rate at which a movement is performed. Speed depends mostly on fast muscle fibres – this is a useful measure in sports such as sprinting, javelin. • Stamina is the ability to keep on exercising for a long time. It would be measured by seeing how long the athlete can continue for – this is a useful measure in X-country, rowing Which measure should be used will depend on the sport.
B.5.3 Distinguish between fast and slow muscle fibres. There are two broad types of voluntary muscle fibers: slow twitch and fast twitch. Slow twitch fibers contract for long periods of time but with little force while fast twitch fibers contract quickly and powerfully but fatigue very rapidly. A.Allott – IB study guide - Biology – Oxford University Press 2007
B.5.5 Discuss the ethics of using performance-enhancing substances, including anabolic steroids. • http://debatepedia.idebate.org/en/index.php/Debate:_Legalization_of_performance-enhancing_drugs_in_pro_sports
B6 - Injuries B.6.1 Discuss the need for warm-up routines. • Here is a PE teachers view: http://www.brianmac.co.uk/warmup.htm • However all evidence for the need to warm up is purely anecdotal and has not been scientifically demonstrated.
B.6.2 Describe injuries to muscles and joints, including sprains, torn muscles, torn ligaments, dislocation of joints and intervertebral disc damage. http://www.doctortipster.com/wp-content/uploads/2011/03/herniated_disc.jpg http://www.healthhype.com/wp-content/uploads/Elbow-Dislocation.jpg http://imaging.ubmmedica.com/shared/zone5/0811JMMCMMF1.jpg http://www.ankleandfootnorthwest.com/images/Ankle%20sprain.jpg http://www.boneclinic.com.sg/wp-content/uploads/2011/06/Ankle-Sprain.jpg