Download
1 / 28
280 likes | 406 Views
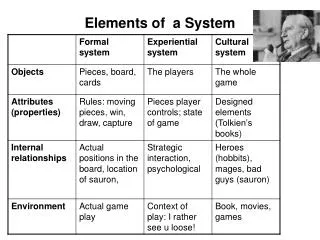
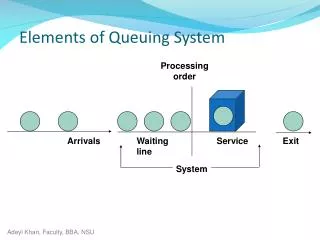
Elements of Health System Financing Lecture 2 of 6. Sources and Means of Health System Finance. Objectives of Second Lecture. Delineate the basic “ sources and means ” or revenue options for health system finance Describe the fundamental features of the different options

E N D
Elements of Health System FinancingLecture 2 of 6 Chernichovsky - Draft
Sources and Means of Health System Finance Chernichovsky - Draft
Objectives of Second Lecture • Delineate the basic “sources and means” or revenue options for health system finance • Describe the fundamental features of the different options • Discuss how well each serves different aims of the health system. Chernichovsky - Draft
Structure of Lecture • Review and introduction • Characteristic of different “sources and means” • Ranking of “sources and means” by their potential impact on relevant health system aims • Summary. Chernichovsky - Draft
Part A: Review and Introduction Chernichovsky - Draft
Noteworthy Points at the Outset • We discuss the potential of financing “elements” and their “options” to achieve “aims”. Bad implementation may foil potential • We do not discuss the element “level of finance” because: • it is largely politically or market determined; that is, it is captured to a substantial extent by sources of financing and their potential to control cost that we do discuss • we wish to focus on the “qualitative” aspects of finance, or how to manage better any “level” • We approximate the aim “health outcomes” by the aim “equity” because the way sources of finance can contribute to health is through: • Risk pooling --- the transfer of funds from the healthy to the sick • Income redistribution --- the transfer of funds from the rich to the poor • Securing that access to care is independent of one’s ability to pay for its full cost. Chernichovsky - Draft
The Basic Matrix: Health System Aims Vs. Financing Elements, Not Including “Level” and “Health”) Chernichovsky - Draft
“Public Financing Principles” • Contributions are • mandatory • Means-tested, rather than • risk-based voluntary premiums or • cost-based voluntary out of pocketfees. …….. • Supports a “standard” package of medical care Chernichovsky - Draft
Part B: Sources and Means of Health System Financing Chernichovsky - Draft
Basic Sources and Means of Health Care Financing • General Revenues • Social Health Insurance (SHI) • The National Pool Model • The National Group Model • The Fragmented Model • ‘Vouchers’ or Medical savings accounts • Private funding • (co-payments in the context of ‘public financing principles’) • Voluntary insurance • Out-of pocket. Chernichovsky - Draft
Relevant Realities • All ‘sources and means’ are found in all systems • There is a dominating source, e.g., private in the USA and poor nations, general revenues in the UK, and Social Insurance in continental Western Europe • The analytic challenge is to examine how the different sources interact. Chernichovsky - Draft
Source I: General Revenues • Revenues from local and central Governments’ tax and fee collections • Revenues not earmarked for medical care but aim to finance care that is: • categorical public entitlement for parts of the population or • universal public entitlement for the entire population • Depend on the tax-base, income-wise and population-wise. There is a problem with the informal sectors mainly in poor developing nations • Reflect national equity and efficiency concerns; will usually be progressive, i.e., tax more the rich and healthy than the poor and sick • Spent while considering government overall priorities, expressed in the budgeting process and its implementation • Paying population has no explicit control over spending patterns. Chernichovsky - Draft
Source II: Social Health Insurance • A group-based arrangement: • The group can from around any institutional basis: work place, union, region, state or nation • The group should not be less than 50,000 members to avoid financial risk associated with unexpectedly high expenditure • Contributions are: • Mandatory • Means-tested rather than risk-based • Earmarked for care of group members • For across-group equity and efficiency, functional (fiscal) federalism needs to be invoked. Chernichovsky - Draft
Types of Social Health Insurance • The National Pool Model • All earmarked contributions for mandated medical care are pooled regionally or nationally (e.g., the Netherlands, Israel, Russia, Colombia) • Across-group equalization is done ex-ante by the national pool • The National Group Model • Earmarked contributions are for mandated care pooled at the group (e.g., Germany, Switzerland) • Across-group equalization is done ex-post • The Fragmented Model • No de-facto national system for mandated care, but groups that collect means-based mandatory contributions to finance care for members (e.g., Mexico) Chernichovsky - Draft
Source III: Vouchers or Medical Savings Accounts • Mandatory tax-exempt contributions of consumers and their employers to a personal earmarked account • Account savings can be used only toward specified care • The client can spend out of his or her pocket on that care beyond the savings amount • Equity and risk-pooling are served by the extent of the tax-exemption or subsidy. Chernichovsky - Draft
Source IV: Private Finance • “Co-payment” • Private payment incurred when consuming care that is public entitlement usually at point of service. Such payments may be “co-insured” • “Out of pocket” • payments based on ability and willingness to pay • Payment for care is at point of service • Voluntary insurance • Individual risk-based premiums paid by the individual or on his behalf, based on expected costs of his care • Community risk-based (averaged for the group) premiums paid by the individual or on his behalf, based on expected costs of the care of the group. Chernichovsky - Draft
Conceptualization of Sources of Health System Finance and Their Features General Revenues Private Insurance Earmarking & risk pooling Mandatory, means-based Social Health Insurance Subsidy Risk pooling Vouchers Out of Pocket Chernichovsky - Draft
Part C:Ranking “sources and means” by their potential impact on relevant health system aims Chernichovsky - Draft
“Sources and Means”: Relevant Health System Aims • Equity (& health) • Macro economic efficiency • (Micro economic efficiency) • Payer (and client) satisfaction. Chernichovsky - Draft
Criteria for Evaluating the Impact of “Source and Means” on Relevant “Aims” • Impact on equity • The potential to pool risk and redistribute income • Impact on macro-economic efficiency • The potential of state and other institutions to control rising cost of medical care • Impact on payer/client satisfaction • Population’s willingness to pay. Chernichovsky - Draft
The Basis for Ranking of Potential“Expert Knowledge” • Theory – economics and other • “Casual” observation • Common knowledge • Judgment. Chernichovsky - Draft
Potential Impact on Equity –(Ordinal Ranking) Chernichovsky - Draft
Potential Impact on Macro Economic Efficiency (Ordinal Ranking) Chernichovsky - Draft
Potential Impact on Micro Economic Efficiency – Collection Cost Chernichovsky - Draft
Potential Impact on Satisfaction of Payers (Ordinal Ranking) Chernichovsky - Draft
Part D: Summary Chernichovsky - Draft
Summary of Potential Impact of Source and Means on Relevant Aims Chernichovsky - Draft
What Next? • The allocation of funds: options and their impact on system aims Chernichovsky - Draft