Download
1 / 4
40 likes | 197 Views
Disseminated Nontuberculous Mycobacterial Infection Mimic Metastases on PET/CT Scan Kuan-Hsiu Lin, MD,* Jao-Hsien Wang, MD,† and Nan-Jing Peng, MD*‡. ( Clin Nucl Med 2008;33: 276–277).

E N D
Disseminated Nontuberculous Mycobacterial Infection Mimic Metastases on PET/CT ScanKuan-Hsiu Lin, MD,* Jao-Hsien Wang, MD,† and Nan-Jing Peng, MD*‡ (Clin Nucl Med 2008;33: 276–277)
Abstract: A 68-year-old man had malaise, weight loss, and enlarged right cervical lymph nodes. The first biopsy from a right cervical lymph node showed granulomas with negative acid-fast bacillus (AFB) staining, and he was treated for extrapulmonary tuberculosis with isoniazid, rifampin, ethambutol, and pyrazinamide. Symptoms persisted even after receiving antituberculosis drugs for 2 months. He was transferred to our center for F-18 FDG PET/CT scan under the suspicion of occult malignancy. The PET/CT scan showed increased FDG uptake in the right cervical lymphadenopathy and multiple bony lesions. The second biopsy from the FDG-avid cervical lymph node and bone marrow confirmed nontuberculous mycobacterial (NTM) infection. After another 6 months of adjusted antituberculosis therapy with isoniazid, rifampin, ethambutol, and clarithromycin, a repeat PET/CT scan showed remission of previous lesions. • Key Words:non-tuberculous mycobacterium (NTM), Mycobacterium kansasii, positron emission tomography.
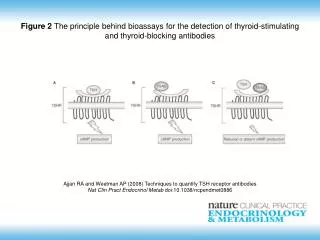
Figure 1 • A 68-year-old man had malaise, weight loss, and enlarged right cervical lymph nodes. The first biopsy from a right cervical lymph node showed granulomas with negative acid-fast bacillus (AFB) staining, and he was treated as for extrapulmonary tuberculosis with isoniazid, rifampin, ethambutol and pyrazinamide. Symptoms persisted even after receiving antituberculosis drugs for 2 months. PET/CT imaging was performed 60 minutes after injection of 444 MBq (12 mCi) F-18 FDG using a GE Discovery LS PET/CT hybrid imaging scanner. Before the study, the patient fasted for 6 hours. It showed increased FDG uptake in right cervical enlarged lymph nodes and multiple bony lesions without obvious destruction involving the spine, rib cage, shoulders, pelvic bones, and femora. The second biopsy from the FDG-avid right cervical node and bone marrow showed granulomas with positive AFB staining, and the culture grew Mycobacterium kansasii. Disseminated nontuberculous mycobacterial (NTM) infection is seldom reported,1 which may mimic malignancy on PET/CT scan.2–7 In this case, PET/CT scan correctly guided biopsy to the exact location of active lesion.
Figure 2 • A repeat FDG/CT scan 6 months later showedremission of prior FDG-avid lesions in the right neck and bones. New osteoblastic reaction without FDG uptake was seen in previous bony lesions.

![Perreault S, et al. Eur J Clin Pharmacol 2009 Jun 16 [Epub]](https://cdn2.slideserve.com/3911021/slide1-dt.jpg)