Download
1 / 43
470 likes | 820 Views
Kidneys and Hypertension. Dr. Shahrzad Shahidi Nephrologist Isfahan University of Medical sciences. Hypertension (HTN). Persistent elevation of arterial blood pressure (BP) 31% of Americans have BP > 140/90 mmHg Most patients asymptomatic

E N D
Kidneys and Hypertension Dr. Shahrzad Shahidi Nephrologist Isfahan University of Medical sciences
Hypertension (HTN) Persistent elevation of arterial blood pressure (BP) 31% of Americans have BP > 140/90 mmHg Most patients asymptomatic Single most preventable cause of premature death in developed countries. Chobanian AV, et al. Hypertension 2003;42(6):1206–1252
Adult Classification Chobanian AV, et al. Hypertension 2003;42(6):1206–1252
Classification for Adults Classification based on average of > 2 properly measured seated BP measurements from > 2 clinical encounters If systolic & diastolic BP values give different classifications, classify by highest category Prehypertension: patients likely to develop hypertension
Pathogenesis. • No one gene is responsible. • Studies shows that several difft genes may have an effect on BP. RARE SINGLE GENE CAUSES OF HTN HAVE BEEN IDENTIFIED.
Single Gene Causes of HTN • Glucocorticoid remediable aldosteronism • Syndrome of minerelocorticoid excess • Pheochromocytoma - may occur with MEN type 2, Von Hippel Lindau disease, Neurofibromatosis type 1 • Liddle’s Syndrome
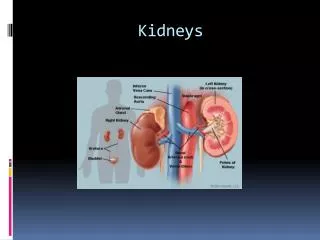
Renin angiotensin system • Renin –secreted by the juxtaglomerular apparatus. • It converts angiotensinogen (inactive) to angiotensin 1 .It then converts to angiotensin 2 by ACE. • Increased renin – RAS, Renal cell carcinoma & rarely some renin secreting tumours.
Actions of angiotensin II • Arteriolar vasoconstriction. • Efferent arteriolar vasocnstriction. • Aldosterone secretion. • Epinephrine release (adrenaline). • Smooth muscle hypertrophy. • Inhibit renin release (negative feed back). • Myocardial growth.
Other pathogenesis • Arterial stiffness – Aging , DM, Kidney disease. • Sympathetic nervous system- Activation associated with sudden rise in BP.- By increasing stroke volume, HR , systemic vascular resistance and activation of RAS.
Secondary Hypertension • Renovascular Disease • Renal parenchymal disease: • CKD • Glomerulonephritis • ADPKD • Obstructive uropathy,…
Renal artery stenosis • Atherosclerotic or fibromuscular dysplasia as etiology • Clinically difficult to control HTN • Renal dysfuntion • Resistant fluid retention • Worsening Cr with ACEI or ARB
Investigations • US Kidneys- assymmetry. • Doppler of renal arteries. • Captopril renogram - affected kidney may show a 30% decline in function. • MRA. • Angiogram- secure diagnosis & allow intervention.
Treatment - in Atheroslerotic RAS • Modify risk factors. • Control BP with loop diretics, CCBs, centrally acting agents, B blockers, • Treatment by angioplasty & stenting OR surgery.
Indications for surgery • Single kidney with stenosis. • Bilateral RAS. • Uncontrolled BP/ flash pulm edema. • Rapidly deteriorating kidney function. • Meaningful nephron mass in the kidneys.
Fibromuscular dysplasia. • Otherwise healthy young women aged 15-50 yrs. • Angiography with “string of beads” pattern • Angioplasy is the treatment.
Fibromuscular Dysplasia, before & after PTRA Atherosclerotic RAS before & after stent Safian & Textor. NEJM 344:6
Initial assessment • Duration of HTN • Other CVD risk factors. • Anything to suggest secondary HTN. (50<Age <30, sudden onset, presents as malignant HTN, sudden deterioration in BP control, resistant HTN)
Initial evaluation • Other contributory factors like –drugs, overweight, Excess alcohol, excess salt intake, Lack of exercise, Environmental stress, smoking. • Evidence of Complications- stroke, TIA, Carotid bruit, IHD, CHF, Cardiomegaly, PVD, Hypertensive retinopathy, Renal impairment, Proteinuria, Sexual dysfunction.
Initial Evaluation • Previous drug treatment and side effects. • Contraindication to specific drugs. • Family history
Initial basic investigations • Hematocrit • FBS • HDL, LDL (after 9-12 h fast) • TG • Cr • K • Ca • Urinalysis • ECG • Optional tests: urinary albumin excretion or ACR
Target organ damage • Heart- LVH, IHD, LVD,CHF. • Brain- Stroke, TIA, Vasular dementia. • Kidney- Chronic Kidney Disease. • Eyes- Retinopathy. • Peripheral Vasculature - Peripheral arterial disease.
Treatment Goals Reduce morbidity & mortality Select drug therapy based on evidence demonstrating risk reduction Chobanian AV, et al. Hypertension 2003;42(6):1206–1252
Lifestyle Modifications DASH, Dietary Approaches to Stop Hypertension
What Drug in CKD • In all proteinuric renal disease ACEI & ARB has a beneficial role. • Dcreases intraglomerular pressure & thus reduce proteinuria. • Dual blockade with ACEI & ARB is a useful combination.
In CKD • Expect the need of 3 meds. • First life style modification. • If proteinuria ACEI or ARB. • If fluid overload diuretics. • If persistant proteinuria add ARB or ACEI. • Last vascular smooth muscle relaxant: Minoxidil
Remember side effects • Hyperkalemia (ACE, ARB) • Fluid retension (Amlodipine) • Bradycardias (B blocker, Clonidine) • Massive fluid overload & Tachycardia (Minoxidil)
Antihypertensives - ACEIs • No ACEI shown to be superior to any other ACEI • 1˚ goal: treat BP to target • 2˚ goal: control proteinuria • ACEIs generally more cost-effective than ARBs • Adverse effects with an ACEI; switch to an ARB may be appropriate
Antihypertensives - ACEIs • Begin at a low dose; increase dose at 4-week intervals to reduce microalbuminuria (even normotensive patients) • Antiproteinuric effects not necessarily attained at antihypertensive doses • Increase dose until proteinuria reduced by 30-50%
Antihypertensives: ARBs • ARBs have similar efficacy to ACEIs for kidney protection in patients with several forms of GN • Proteinuria reduction: 25 to 47% • Most clinicians use ACEI/ARB therapy in patients with nondiabetic CKD & proteinuria
Antihypertensives: ARBs • Selection of ACEIs vs ARBs • Cost of therapy • Patient tolerance • Clinician preference
Nondihydropyridine CCBs • Diltiazem/verapamil decrease glomerular injury without negatively changing renal hemodynamics • May have beneficial effects on proteinuria similar to ACEIs
Nondihydropyridine CCBs • Studies suggest efficacy of combination therapy with ACEIs & nondihydropyridine CCBs may be superior in proteinuria reduction than either agent alone • Generally 2nd line when ACEIs or ARBs not tolerated
Speculations on JNC VIII • Diuretics will remain first line therapy • Chlorthalidone vs. HCTZ • Beta blockers will be dropped to 2nd or 3rd line therapy • Combination RAAS inhibition may carry more risk than benefit and will probably not be recommended (some exceptions) • Strong emphasis on combination therapy