Download
1 / 1
10 likes | 165 Views
Imaging of the Urinary Tract at VAMC: Optimizing Utilization of CTU and IVP M.A. Rischall, MD , N.R. Mraz , MD. Department of Radiology, University of Minnesota, Minneapolis, Minnesota. VA urology clinicians order an average of 151 IVP/yr ( StDev 29), 1024 CTU/yr ( StDev

E N D
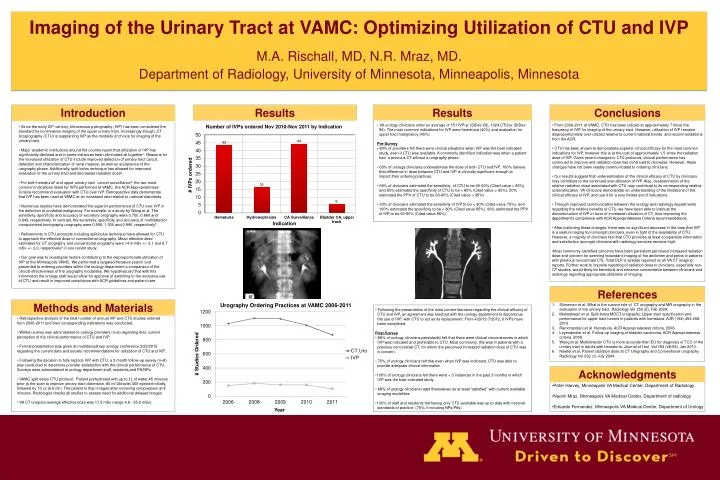
Imaging of the Urinary Tract at VAMC: Optimizing Utilization of CTU and IVP M.A. Rischall, MD, N.R. Mraz, MD. Department of Radiology, University of Minnesota, Minneapolis, Minnesota • VA urology clinicians order an average of 151 IVP/yr (StDev 29), 1024 CTU/yr (StDev • 96).The most common indications for IVP were hematuria (40%) and evaluation for • upper tract malignancy (45%) • Pre-Survey • 80% of providers felt there were clinical situations when IVP was the best indicated • study, even if CTU was available. A commonly identified indication was when a patient • had a previous CT without a urography phase. • 60% of urology clinicians underestimate the dose of both CTU and IVP. 100% believe • that difference in dose between CTU and IVP is clinically significant enough to • impacttheir ordering practices. • 66% of clinicians estimated the sensitivity of CTU to be 40-60% (Cited value > 95%) • and 83% estimated the specificity of CTU to be < 80% (Cited value > 95%). 50% • estimated the PPV of CTU to be 60-80% (Cited value > 95%) • 33% of clinicians estimated the sensitivity of IVP to be < 60% (Cited value 75%), and • 100% estimated the specificity to be < 80% (Cited value 85%). 66% estimated the PPV • of IVP to be 60-80% (Cited value 85%). • From 2006-2011 at VAMC, CTU has been utilized at approximately 7 times the frequency of IVP for imaging of the urinary tract. However, utilization of IVP remains disproportionately over-utilized relative to current national trends and recommendations from the ACR. • CTU has been shown to demonstrate superior clinical efficacy for the most common indications for IVP, however this is at the cost of approximately 1.5 times the radiation dose of IVP. Given recent changes in CTU protocols, clinical performance has continued to improve and radiation dose has continued to decrease. However, these changes have not been readily communicated to ordering clinicians. • Our results suggest that underestimation of the clinical efficacy of CTU by clinicians may contribute to the continued overutilization of IVP. Also, overestimation of the relative radiation dose associated with CTU may contribute to its corresponding relative underutilization. VA clinicians demonstrate an understanding of the limitations of the clinical efficacy of IVP, and use it for a very limited set of indications. • Through improved communication between the urology and radiology departments regarding the relative benefits of CTU, we have been able to institute the discontinuation of IVP in favor of increased utilization of CT, thus improving the department’s compliance with ACR Appropriateness Criteria recommendations. • After instituting these changes, there was no significant decrease in the view that IVP is a useful imaging tool amongst clinicians, even in light of the availability of CTU. However, a majority of clinicians feel that CTU provides at least comparable information and satisfaction amongst clinicians with radiology services remains high. • Most commonly identified concerns have been persistent perceived increased radiation dose and concern for seeming redundant imaging of the abdomen and pelvis in patients with previous noncontrastCTs. Total DLP is already reported on all VA CT imaging reports. Further work to improve reporting of radiation dose to clinicians, especially non-CT studies, would likely be beneficial and enhance concordance between clinicians and radiology regarding appropriate utilization of imaging. • Since the early 20th century, Intravenous pyelography (IVP) has been considered the standard for noninvasive imaging of the upper urinary tract. Increasingly though, CT Urogrography (CTU) is supplanting IVP as the modality of choice for imaging of the urinary tract. • Major academic institutions around the country report that utilization of IVP has significantly declined and in some instances been eliminated all together1. Reasons for the increased utilization of CTU include improved detection of urinary tract calculi, detection and characterization of renal masses, as well as acceptance of the urography phase. Additionally, split-bolus technique has allowed for improved evaluation of the urinary tract and decreased radiation dose2. • For both hematuria3 and upper urinary tract cancer surveillance4, the two most common indications listed for IVPs performed at VAMC, the ACR Appropriateness Criteria recommend evaluation with CTU over IVP. Retrospective data demonstrate that IVP has been used at VAMC at an increased rate relative to national standards. • Numerous studies have demonstrated the superior performance of CTU over IVP in the detection of urothelial malignancy. For example, in a study by Wang et al. The sensitivity, specificity and accuracy of excretory urography were 0.750, 0.860 and 0.849, respectively. In contrast, the sensitivity, specificity and accuracy of multidetector computerized tomography urography were 0.958, 1.000 and 0.996, respectively5. • Refinements in CTU protocols including split-bolus technique have allowed for CTU to approach the effective dose of conventional urography. Mean effective dose estimates for CT urography and conventional urography were 14.8 mSv +/- 3.1 and 9.7 mSv +/- 3.0, respectively6 in one recent study. • Our goal was to investigate factors contributing to the disproportionate utilization of IVP at the Minneapolis VAMC. We performed a targeted literature search and presented to ordering providers within the urology department a comparison of the clinical effectiveness of the urography modalities. We hypothesized that with this information the urology staff would allow for approval of switching to the exclusive use of CTU and result in improved compliance with ACR guidelines and patient care. References Introduction Results Results Conclusions Methods and Materials Acknowledgments • Silverman et al. What is the current role of CT urography and MR urography in the evaluation of the urinary tract. Radiology Vol 250 (2), Feb 2009. • Maheshwari et al. Split-bolus MDCT urography: Upper tract opacification and performance for upper tract tumors in patients with hematuria. AJR (194) 453-458. 2010. • Ramchandani et al. Hematuria. ACR Appropriateness criteria. 2008. • Leyendecker et al. Follow-up imaging of bladder carcinoma. ACR Appropriateness criteria. 2009. • Wang et al. Multidetector CTU is more accurate than EU for diagnosis of TCC of the urinary tract in adults with hematuria. Journal of Urol. Vol 183 (48-55). Jan 2010. • Nawfel et al. Patient radiation dose at CT Urography and Conventional urography. Radiology Vol 232 (1) July 2004. • Following the presentation of the most current literature regarding the clinical efficacy of • CTU and IVP, an agreement was reached with the urology department to discontinue • the use of IVP, with CTU to act as its replacement. From 4/2012-7/2012, 0 IVPshave • been completed. • Post-Survey • 88% of urology clinicians persistently felt that there were clinical circumstances in which • IVPwas indicated and preferable to CTU. Most commonly, this was in patients with a • previous noncontrast CT, for whom the perceived increased radiation dose of CTU was • a concern. • 75% of urology clinicians felt that even when IVP was indicated, CTU was able to • provide adequate clinical information • 100% ofurology clinicians felt there were < 3 instances in the past 3 months in which • IVP was the best indicated study. • 88% of urology clinicians rated themselves as at least “satisfied” with current available • imaging modalities • 100% of staff and residents felt having only CTU available was up to date with national • standards of practice. (75% if including NPs/PAs) • Retrospective analysis of the total number of annual IVP and CTU studies ordered from 2006-2011 and their corresponding indications was conducted. • Written survey was administered to urology providers (n=6) regarding their current perception of the clinical performance of CTU and IVP. • Formal presentation was given at multidisciplinary urology conference 3/23/2012 regarding the current data and society recommendations for utilization of CTU and IVP. • Following the decision to fully replace IVP with CTU, a 3 month follow-up survey (n=8) was conducted to determine provider satisfaction with the clinical performance of CTU. Surveys were administered to urology department staff, residents and PA/NPs. • VAMC split-bolus CTU protocol: Patient prehydrated with up to 1L of water 45 minutes prior to the scan to improve urinary tract distension. 80 ml Ultravist 300 injected initially, followed by 70 cc at 6 min. The patient is than imaged after removing compression at 8 minutes. Radiologist checks all studies to assess need for additional delayed images • VA CT urogram average effective dose was 17.2 mSv (range 4.8 - 55.2 mSv). • Peter Harvey, Minneapolis VA Medical Center, Department of Radiology • Naomi Mraz, Minneapolis VA Medical Center, Department of radiology • Eduardo Fernandez, Minneapolis VA Medical Center, Department of Urology