Download
1 / 23
230 likes | 345 Views
Comprehensive Complex Care Model for Central Oregon An Innovative Community Collaborative. Patient Story.

E N D
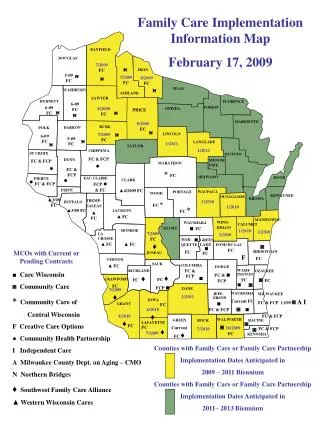
Comprehensive Complex Care Model for Central Oregon An Innovative Community Collaborative
Patient Story Rebecca is a 53-year-old patient who moved to Prineville a few years ago. She came to Mosaic with multiple medical issues including Type 2 diabetes, high blood pressure and the effects from a debilitating stroke a few years ago. Additionally she had severe social anxiety, depression and had made multiple suicide attempts. Rebecca’s Mosaic provider began by sorting out her 28 medications and multiple medical issues while a Community Health Worker (CHW) helped Rebecca start the process to sign up for Medicaid. The CHW also started helping her look for housing and furniture to go with it so she could get out of an unsupportive home situation. Rebecca also started seeing the Mosaic behavioral health consultant for her anxiety and depression. Additionally, the Mosaic RN Care Coordinator started checking in with her monthly to help her manage her diabetes With all these team efforts, Rebecca’s mental and physical health started improving drastically. The behavioral health consultant and the CHW went so far as to work with Rebecca’s new housing manager to help her keep a dog for mental health support in her new apartment. Rebecca is also successfully checking her own blood sugar for the first time in many years.
Central Oregon Complex Care Strategy –Centered Around the Patient Customized Comprehensive Eval Team-based Care Proactive, between visit care Shared Action Plan Actionable data in the hands of caregivers Pharmacy Management Community Collaborative Patient Transitions of Care Socio-behavioral Risk Modification Multi-faceted Approach Patient Education Specialist Coordination Virtual Visits Nutrition Counseling
Developing a Complex Care Strategy:Serving Rebecca, Addressing Community Opportunity
A Community Vision Part of a journey towards better health and sustainability for Central Oregon
Bridges HealthSupporting Patients and Providers Vision: World class complex care center coupled with strong distributed network of services to provide community with comprehensive model • Primary Care referral center for complex and intensive care (Ambulatory ICU): Comprehensive care for patients including primary care, behavioral health, social work, physical therapy, pain, nutrition, education, etc. • An “Innovation Hub”; Starting point for a robust community strategy: developing workforce and competencies --- helping the medical groups build internal competencies; delivering high dose of intervention in the central location, and expanding to a distributed model • A Community Referral Point - Patients would be referred by their primary care physician to seek care at the Complex Care Center – where they would meet a physician and integrated team to address health (and life) needs. Strong communication processes with the referring physician would be hardwired • Patient-led: A spirit of patient-centeredness would be embodied in the care model, the staffing, cultural sensitivities. More formally, a patient advisory council is being formed
The Basics What: Develop a comprehensive complex care strategy, a component of which is a dedicated outpatient complex care clinic called Bridges Health When: Open Bridges Health in August 2013, with evolution of community distributed complex care services between now and go live Who: A community collaborative, with an investment from PacificSource and Mosaic as an operating partner. Led by advisors to guide the innovation and spread. How: Two pronged approach: • Centralized: a center with physicians, nurses, health coaches, behavioral health specialists, pharmacy, community health workers, and pain specialists providing comprehensive complex care to 1600-2000 members of our community • Distributed: provision of community resources to support complex care needs within community practices in more dispersed geographic areas Where: PacificSource Building, near the St Charles campus, directly above the St. Charles Family Care clinic
Bridges Health Benefits for the Patient • A dedicated Bridges Health team member to: • Engage with the patient and support their care needs, concerns, answer questions and provide education • Support care and partner with the patient in providing comprehensive access to meet their healthcare needs • Facilitate and enable effective communication across the continuum for the patient • Be a health coach and guide the patient in meeting his/her goals, motivating the patient to take steps towards improved health • Additional team resources include behavioral health, pharmacy, pain management, community health coaching, etc. – all with partnership with the Bridges Health Medical Directors • 24/7 access to Bridges Health team via phone, email or in person • Bridges Health enables an engaged community of family / caregivers • Holistic care that centers on bettering the patient as a whole – physical and mental health, community resources, family services, etc.
Provider Feedback From Initial Eligible Patient Review • High burden of clinical conditions • Significant level of social and behavioral health challenges • Claims review identifies frequent utilization unknown to PCP • Significant gaps in care – especially Rx adherence • Recognition that these patients are challenging and often not progressing in health – however unclear pathway on how to change that paradigm • Recognition that many identified patients have “stable chronic conditions”
Key Success Elements • Analytics – Data/Metrics – Targeted population • Patients with persistent and Actionable disease, disease burden or utilization pattern • Opportunity for outcomes impact, meaningful patient service and financial sustainability rests on identifying the right members; predictive model + clinical intelligence rules + utilization triggers • Other Analytics – Data/Metrics • Enhanced Data Transparency • Robust evaluation of the model to understand effectiveness of model • Member Engagement • Care model to “meet patients where they are” • clear articulation of value; open access; superb service; “Surprise and delight” elements, smooth transitions; no additional cost to member • Primary referral source will be the patients’ community PCP; members without PCPs may be invited in through other mechanisms • PCP key referral source and most trusted relationship for most patients. • Strong communications key to transitions, co-management of patients
Essential Care Model Elements • Complex Care Model • Dedicated Team-Based Care: • MD + Care Manager + Multi-disciplinary team • Supervisit • Initial visit sets shared trust • Shared Action Plan • Standard, active, dynamic document keeps everyone on same page • Rules-based Proactive Care Management • Ongoing proactive care partnership with patient • Bridges Health Payment Model • Beyond Fee For Service Reimbursement at Center; Shared Incentive to Community Providers • Community/Provider Partnership Development • To facilitate transitions, appropriate use of community resources • Communications • Thoughtfully developed patient communication materials to achieve targeted enrollment in Bridges Health • Space Readiness: Design and Buildout • Develop a patient centered space to achieve optimal patient engagement
Bridges Health Staffing Model Dedicated Team: • Bridges Health Medical Director • Bridges Health Clinic Administrator • 1 Additional Physician • 1 Nurse Practitioner • 3 Care Managers • 4 Community Health Workers • 1 Administrative Assistant • 1 Receptionist • Social Worker that can provide behavioral health services • Additional Behavioral Health Specialist with prescribing capabilities • Pharmacist • Nutritionist
Bridges Health Patient Identification Process PacificSourcewill use specific risk modeling tools to identify eligible Bridges Health patients using claims data. Patients will also be referred into Bridges Health by their primary care providers using specific defined criteria or following a health event (e.g. hospitalization). Specific variables for risk identification include: • Diagnostic Criteria • Comorbid Behavioral Health Accelerators • Provider Referral • Patient Wellness Assessments • Truven Prospective Risk Scores • Diagnostic detail • Demographics • Claims Experience • Inpatient Experience • ED Experience
Supervisit Philosophy A key success element for Bridges Health is the initial patient on-boarding and first visit with the Care Coordinator, Bridges Health Medical Director and the Patient • Provides an opportunity for MD, Care Coordinator and patient to share trust • Provides platform for deeply assessing patient’s health and multi-domain assessment of life challenges getting in the way of achieving optimal health • Enables start of Action Plan • Allows for longer face-to-face time, which later facilitates email and telephonic interactions • Provides (and forces) an intentional, structured opportunity to discuss many of the patient’s goals/concerns
Supervisit Timeline - Intensivist Model Total Time = ~ 1hour and 30 minutes Patient Time: 60 minutes Care Coordinator Time: ~90 minutes Intensivist Time: 45-60 minutes Pre-visit planning 15-20 min Care Coord - Patient end visit 15-20 min Care Coordinator, Intensivist and Patient visit 45-60 min
Domains for Assessment A critical goal of the Supervisit is to evaluate the patient for areas of risk, so that you may over time together develop actions steps to address risks. Examples of risk areas include: • Medical Risk Domains – Complexity of disease, complexity of treatment, unstable disease, etc. • Behavioral Risk Domains • Social Risk Domains • Utilization/Access Risk Domains • Functioning Risks: Physical Functioning Risks • Self-efficacy, Confidence Risks (including an assessment of Patient Activation)
Bridges and Referring PCP Have Close Communication Channels The Bridges Health team serves as a referral extension to the community PCP. As such – the Bridges Health team commits to regular communication and updates to the referring PCP, and also will look for input and feedback from the referring PCP as the patient receives care at Bridges. • Template Referral tool and process • Pre-Supervisit planning agenda • Post-Supervisit communication • Shared Action Plan • Ongoing structured communication • Graduation templated communication • Open access for discussion
Where the Savings Accrue Modeling savings: 600 Medicare members in complex care
Complex Care Model PCP Level Economics for Referrals to Complex Care FFS Revenue Shift Risk Model Economics* • 5% savings on 1600 Complex Patients = $2M • 10% Savings = $2M • 5% Savings Spread among 400 COIPA Providers = $5,000/pt. • 10% = $10,000/pt. PSHP Medicare Top 10% PSHP Commercial Top 10% PSHP Medicaid Top 10% $35 PMPM $70 PMPM $30 PMPM PCP Practice • Payor Mix 60% Medicaid/30% Medicare/ 10% Commercial • $45 PMPM revenue shift • $540 Annual revenue loss Estimated return to PCP per patient referral:* 9:1 to 18:1 *Assumes minimum medical loss ratio targets are achieved during contract year
Impact on PCP office Soft Costs Avoided • Front office burden • No show rate and noncompliance • Frequent Rx refills and other requests • Staff burnout • Narcotic management